

Evolution of Eczema, Wheeze, and Rhinitis from Infancy to Early Adulthood: Four Birth Cohort Studies
- PMID: 35679320
- PMCID: PMC9802000
- DOI: 10.1164/rccm.202110-2418OC
Evolution of Eczema, Wheeze, and Rhinitis from Infancy to Early Adulthood: Four Birth Cohort Studies
Abstract
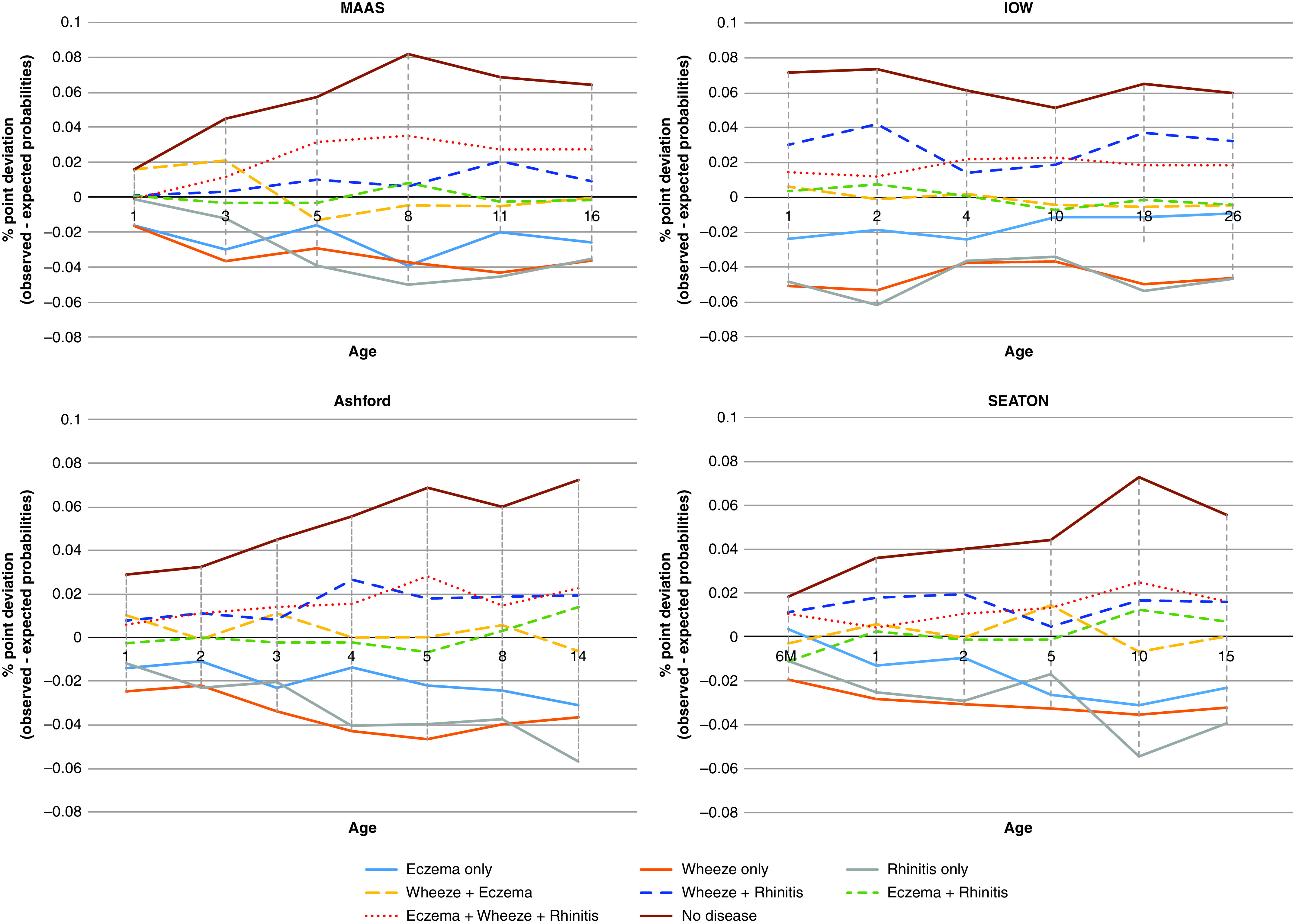
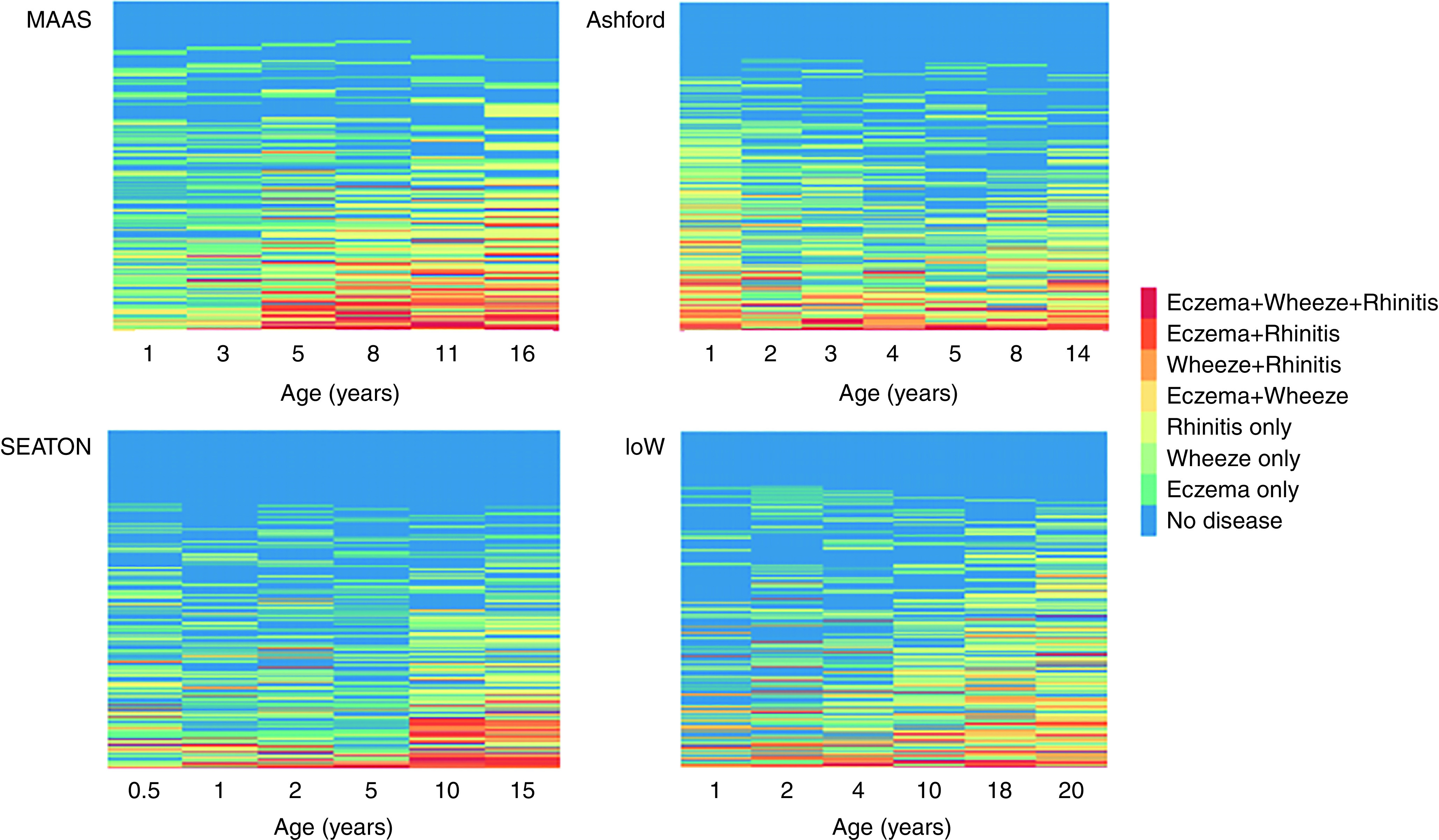
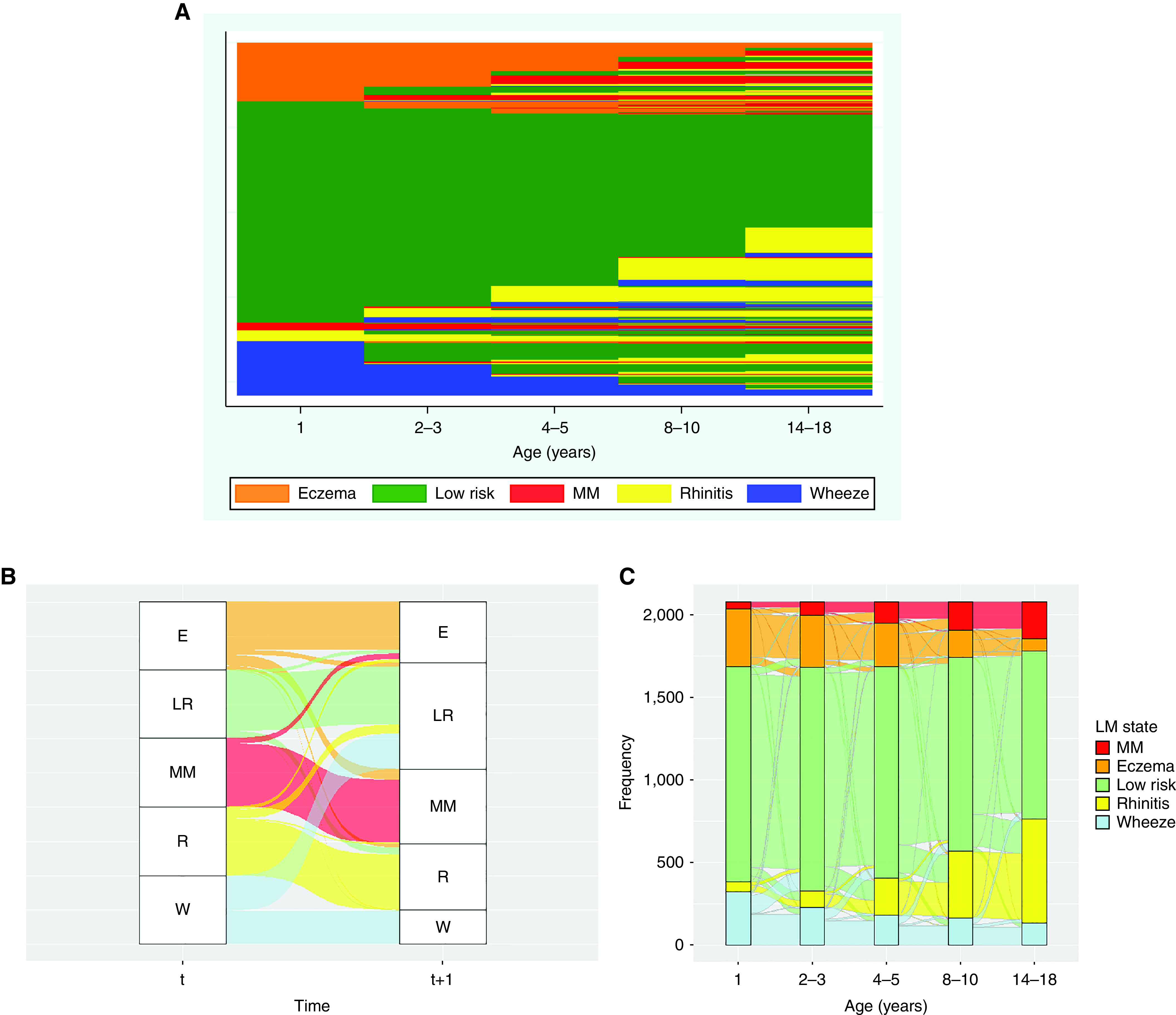
Rationale: The relationship between eczema, wheeze or asthma, and rhinitis is complex, and epidemiology and mechanisms of their comorbidities is unclear. Objectives: To investigate within-individual patterns of morbidity of eczema, wheeze, and rhinitis from birth to adolescence/early adulthood. Methods: We investigated onset, progression, and resolution of eczema, wheeze, and rhinitis using descriptive statistics, sequence mining, and latent Markov modeling in four population-based birth cohorts. We used logistic regression to ascertain if early-life eczema or wheeze, or genetic factors (filaggrin [FLG] mutations and 17q21 variants), increase the risk of multimorbidity. Measurements and Main Results: Single conditions, although the most prevalent, were observed significantly less frequently than by chance. There was considerable variation in the timing of onset/remission/persistence/intermittence. Multimorbidity of eczema+wheeze+rhinitis was rare but significantly overrepresented (three to six times more often than by chance). Although infantile eczema was associated with subsequent multimorbidity, most children with eczema (75.4%) did not progress to any multimorbidity pattern. FLG mutations and rs7216389 were not associated with persistence of eczema/wheeze as single conditions, but both increased the risk of multimorbidity (FLG by 2- to 3-fold, rs7216389 risk variant by 1.4- to 1.7-fold). Latent Markov modeling revealed five latent states (no disease/low risk, mainly eczema, mainly wheeze, mainly rhinitis, multimorbidity). The most likely transition to multimorbidity was from eczema state (0.21). However, although this was one of the highest transition probabilities, only one-fifth of those with eczema transitioned to multimorbidity. Conclusions: Atopic diseases fit a multimorbidity framework, with no evidence for sequential atopic march progression. The highest transition to multimorbidity was from eczema, but most children with eczema (more than three-quarters) had no comorbidities.
Keywords: asthma; atopic march; birth cohorts; eczema; wheeze.
Figures
Comment in
-
Revisiting the Atopic March Current Evidence.Am J Respir Crit Care Med. 2022 Oct 15;206(8):925-926. doi: 10.1164/rccm.202206-1219ED. Am J Respir Crit Care Med. 2022. PMID: 35816436 Free PMC article. No abstract available.
-
Modeling the Natural Course of Atopic Multimorbidity: Correlates of Early-Life States and Exposures.Am J Respir Crit Care Med. 2023 Mar 1;207(5):633-634. doi: 10.1164/rccm.202211-2062LE. Am J Respir Crit Care Med. 2023. PMID: 36480962 Free PMC article. No abstract available.
-
IgE Sensitization Drives the Atopic March.Am J Respir Crit Care Med. 2023 Mar 1;207(5):632-633. doi: 10.1164/rccm.202210-2022LE. Am J Respir Crit Care Med. 2023. PMID: 36480963 Free PMC article. No abstract available.
-
New Evidence on the Development of Atopic Multimorbidity: Are Patients Marching to the Beat of Their Own Drum?J Allergy Clin Immunol Pract. 2023 Aug;11(8):2620-2621. doi: 10.1016/j.jaip.2023.05.032. J Allergy Clin Immunol Pract. 2023. PMID: 37558364 No abstract available.
References
-
- Moreno MA. JAMA pediatrics patient page: atopic diseases in children. JAMA Pediatr . 2016;170:96. - PubMed
-
- Custovic A, Custovic D, Kljaić Bukvić B, Fontanella S, Haider S. Atopic phenotypes and their implication in the atopic march. Expert Rev Clin Immunol . 2020;16:873–881. - PubMed
-
- Custovic A, Henderson J, Simpson A. Does understanding endotypes translate to better asthma management options for all? J Allergy Clin Immunol . 2019;144:25–33. - PubMed
-
- Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol . 2019;123:144–151. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
