

Patient and Provider Web-Based Decision Support for Breast Cancer Chemoprevention: A Randomized Controlled Trial
- PMID: 35679576
- PMCID: PMC9532364
- DOI: 10.1158/1940-6207.CAPR-22-0013
Patient and Provider Web-Based Decision Support for Breast Cancer Chemoprevention: A Randomized Controlled Trial
Abstract
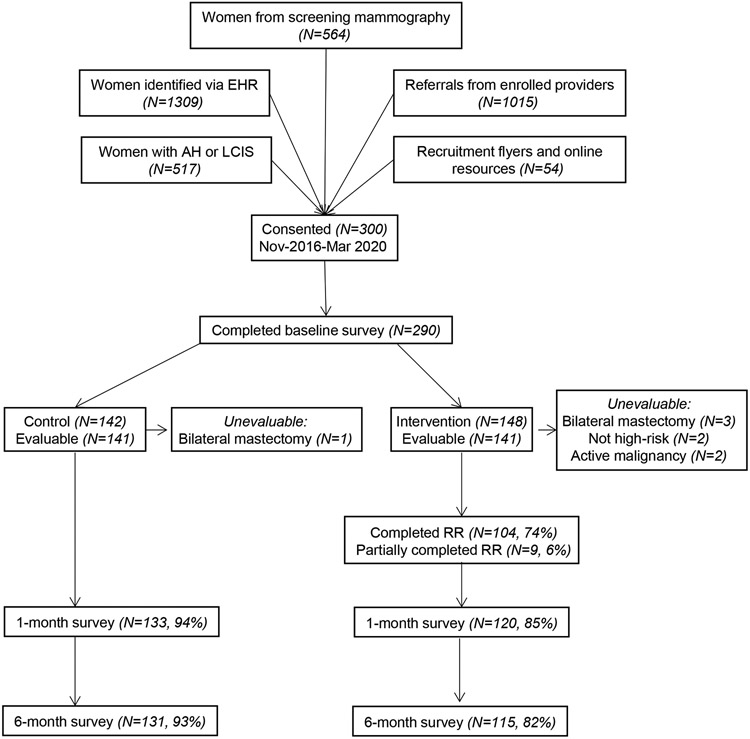
Significant underutilization of breast cancer chemoprevention remains, despite guidelines stating that physicians should recommend chemoprevention with antiestrogen therapy to high-risk women. We randomized women, ages 35 to 75 years, who met high-risk criteria for breast cancer, without a personal history of breast cancer or prior chemoprevention use, to standard educational materials alone or combined with a web-based decision aid. All healthcare providers, including primary care providers and breast specialists, were given access to a web-based decision support tool. The primary endpoint was chemoprevention uptake at 6 months. Secondary outcomes included decision antecedents (perceived breast cancer risk/worry, chemoprevention knowledge, self-efficacy) and decision quality (decision conflict, chemoprevention informed choice) based upon patient surveys administered at baseline, 1 and 6 months after randomization. Among 282 evaluable high-risk women enrolled from November 2016 to March 2020, mean age was 57 years (SD, 9.9) and mean 5-year invasive breast cancer risk was 2.98% (SD, 1.42). There was no significant difference in chemoprevention uptake at 6 months between the intervention and control groups (2.1% vs. 3.5%). Comparing the intervention and control arms at 1 month, there were significant differences among high-risk women in accurate breast cancer risk perceptions (56% vs. 39%, P = 0.017), adequate chemoprevention knowledge (49% vs. 27%, P < 0.001), mean decision conflict (34.0 vs. 47.0, P < 0.001), and informed choice (41% vs. 23%, P = 0.003). These differences were no longer significant at 6 months. Although our decision support tools did not result in a significant increase in chemoprevention uptake, we did observe improvements in decision antecedents and decision quality measures.
Prevention relevance: In this randomized controlled trial of decision support for 300 high-risk women and 50 healthcare providers, we did not observe a significant increase in chemoprevention uptake, which remained low at under 5%. However, these decision support tools may increase knowledge and informed choice about breast cancer chemoprevention.
©2022 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A: Cancer Statistics, 2021. CA Cancer J Clin 2021, 71(1):7–33. - PubMed
-
- Fisher B, Costantino JP, Wickerham DL, Cecchini RS, Cronin WM, Robidoux A et al. : Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst 2005, 97(22):1652–1662. - PubMed
-
- Goss PE, Ingle JN, Ales-Martinez JE, Cheung AM, Chlebowski RT, Wactawski-Wende J et al. : Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med 2011, 364(25):2381–2391. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
