

Cervical lymph nodes and ovarian teratomas as germinal centres in NMDA receptor-antibody encephalitis
- PMID: 35680425
- PMCID: PMC9486890
- DOI: 10.1093/brain/awac088
Cervical lymph nodes and ovarian teratomas as germinal centres in NMDA receptor-antibody encephalitis
Abstract
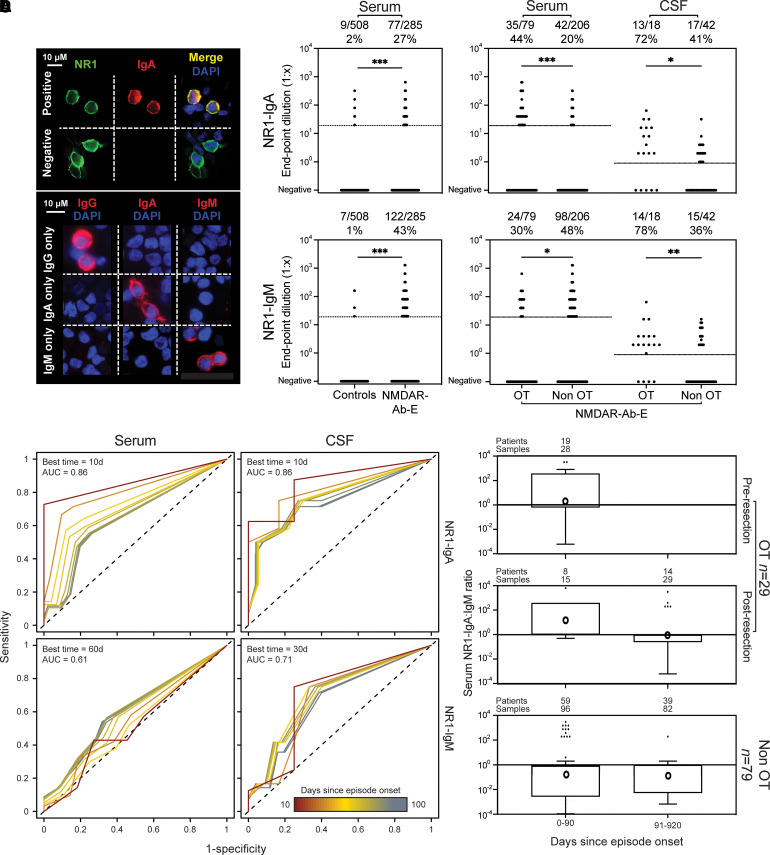
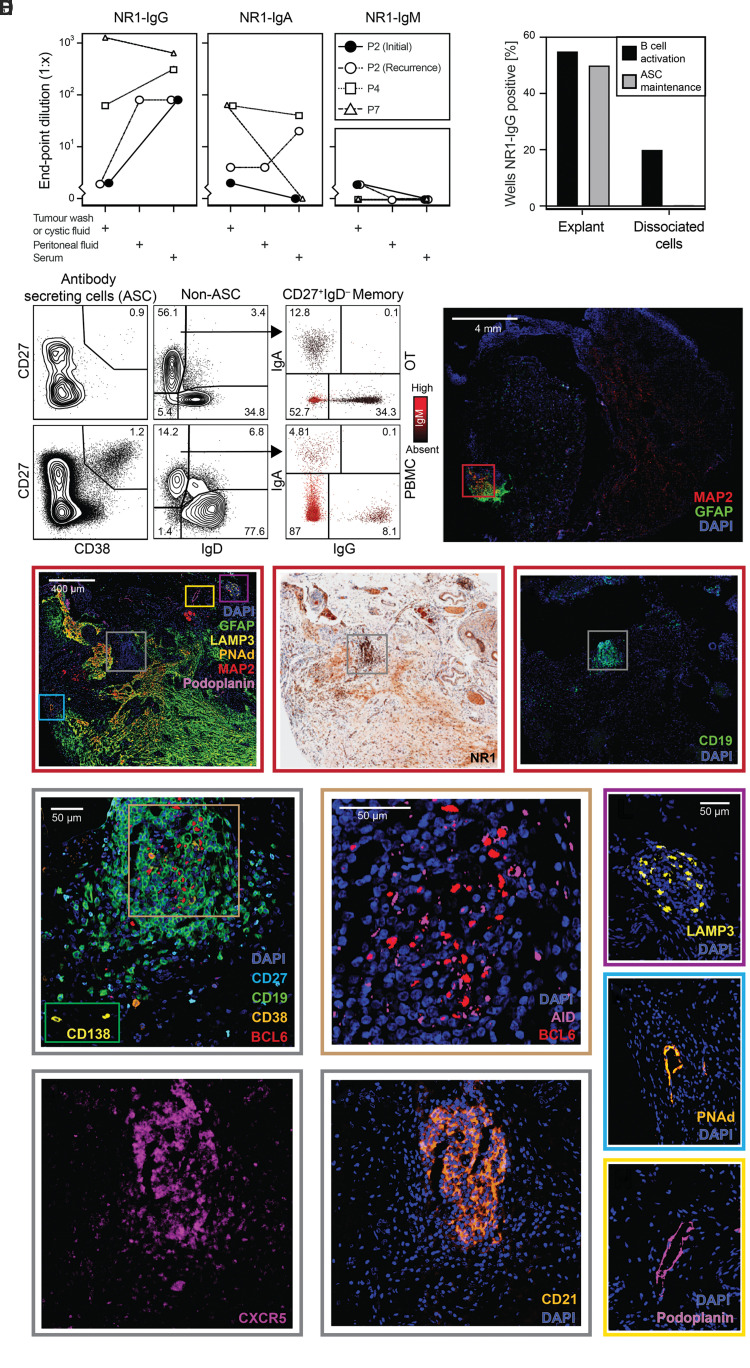
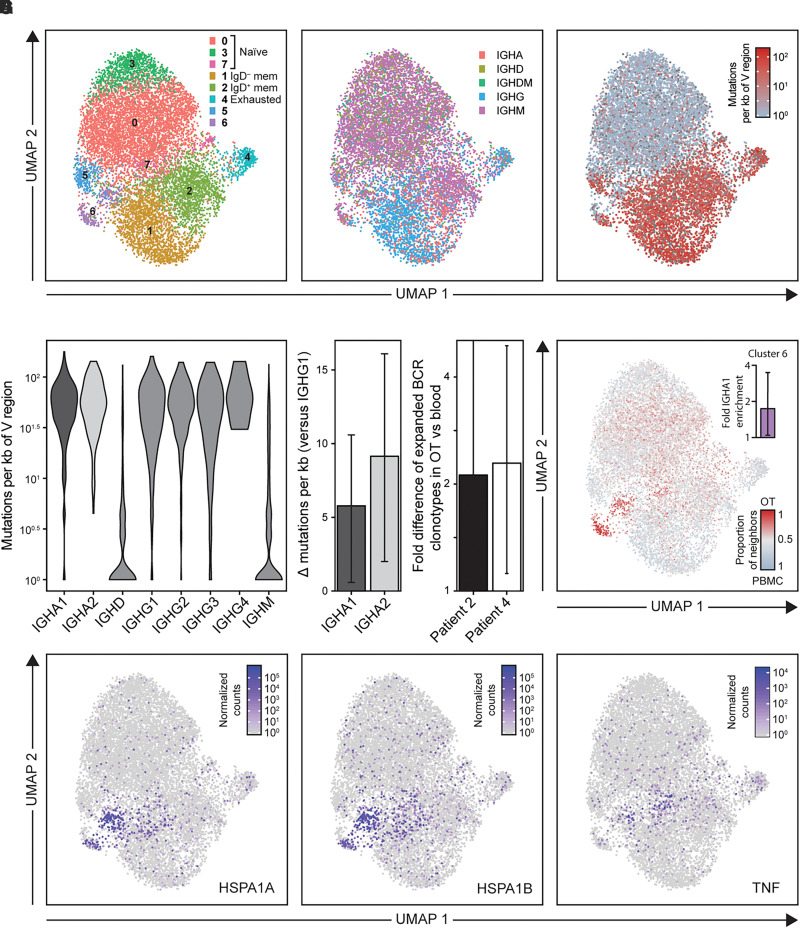
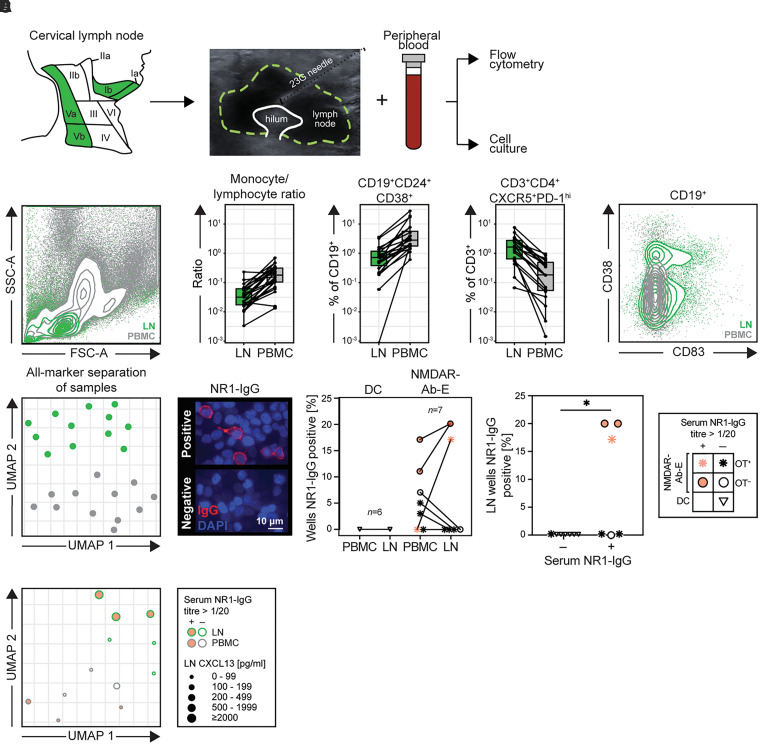
Autoantibodies against the extracellular domain of the N-methyl-d-aspartate receptor (NMDAR) NR1 subunit cause a severe and common form of encephalitis. To better understand their generation, we aimed to characterize and identify human germinal centres actively participating in NMDAR-specific autoimmunization by sampling patient blood, CSF, ovarian teratoma tissue and, directly from the putative site of human CNS lymphatic drainage, cervical lymph nodes. From serum, both NR1-IgA and NR1-IgM were detected more frequently in NMDAR-antibody encephalitis patients versus controls (both P < 0.0001). Within patients, ovarian teratoma status was associated with a higher frequency of NR1-IgA positivity in serum (OR = 3.1; P < 0.0001) and CSF (OR = 3.8, P = 0.047), particularly early in disease and before ovarian teratoma resection. Consistent with this immunoglobulin class bias, ovarian teratoma samples showed intratumoral production of both NR1-IgG and NR1-IgA and, by single cell RNA sequencing, contained expanded highly-mutated IgA clones with an ovarian teratoma-restricted B cell population. Multiplex histology suggested tertiary lymphoid architectures in ovarian teratomas with dense B cell foci expressing the germinal centre marker BCL6, CD21+ follicular dendritic cells, and the NR1 subunit, alongside lymphatic vessels and high endothelial vasculature. Cultured teratoma explants and dissociated intratumoral B cells secreted NR1-IgGs in culture. Hence, ovarian teratomas showed structural and functional evidence of NR1-specific germinal centres. On exploring classical secondary lymphoid organs, B cells cultured from cervical lymph nodes of patients with NMDAR-antibody encephalitis produced NR1-IgG in 3/7 cultures, from patients with the highest serum NR1-IgG levels (P < 0.05). By contrast, NR1-IgG secretion was observed neither from cervical lymph nodes in disease controls nor in patients with adequately resected ovarian teratomas. Our multimodal evaluations provide convergent anatomical and functional evidence of NMDAR-autoantibody production from active germinal centres within both intratumoral tertiary lymphoid structures and traditional secondary lymphoid organs, the cervical lymph nodes. Furthermore, we develop a cervical lymph node sampling protocol that can be used to directly explore immune activity in health and disease at this emerging neuroimmune interface.
Keywords: NMDAR-antibody encephalitis; brain autoimmunity; cervical lymph node; germinal centre; teratoma.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
