

The assessment of antimalarial drug efficacy in vivo
- PMID: 35680541
- PMCID: PMC7613059
- DOI: 10.1016/j.pt.2022.05.008
The assessment of antimalarial drug efficacy in vivo
Abstract
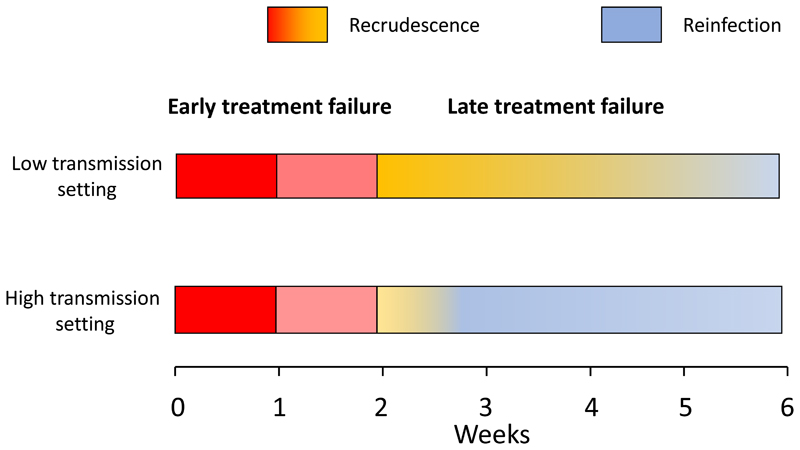
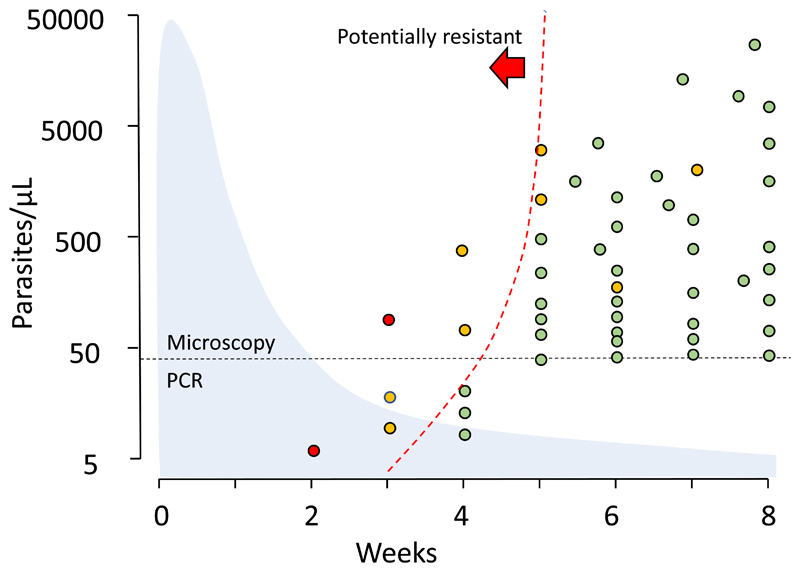
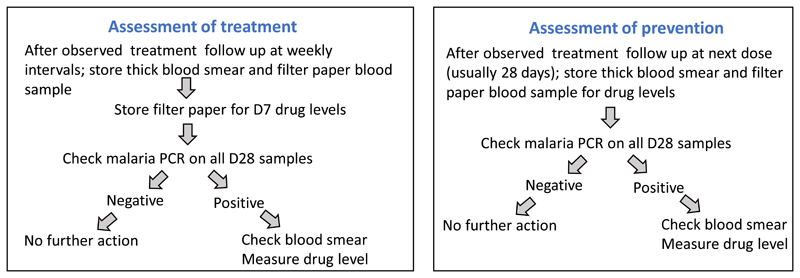
Currently recommended methods of assessing the efficacy of uncomplicated falciparum malaria treatment work less well in high-transmission than in low-transmission settings. There is also uncertainty how to assess intermittent preventive therapies and seasonal malaria chemoprevention (SMC), and Plasmodium vivax radical cure. A pharmacometric antimalarial resistance monitoring (PARM) approach is proposed specifically for evaluating slowly eliminated antimalarial drugs in areas of high transmission. In PARM antimalarial drug concentrations at recurrent parasitaemia are measured to identify outliers (i.e., recurrent parasitaemias in the presence of normally suppressive drug concentrations) and to evaluate changes over time. PARM requires characterization of pharmacometric profiles but should be simpler and more sensitive than current molecular genotyping-based methodologies. PARM does not require parasite genotyping and can be applied to the assessment of both prevention and treatment.
Keywords: antimalarial drugs; chemoprevention; malaria; pharmacometric antimalarial resistance monitoring (PARM); pharmacometrics; treatment.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests The author declares no competing interests.
Figures

Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Examining Plasmodium falciparum and P. vivax clearance subsequent to antimalarial drug treatment in the Myanmar-China border area based on quantitative real-time polymerase chain reaction.BMC Infect Dis. 2016 Apr 16;16:154. doi: 10.1186/s12879-016-1482-6. BMC Infect Dis. 2016. PMID: 27084511 Free PMC article.
-
Risk of Plasmodium vivax parasitaemia after Plasmodium falciparum infection: a systematic review and meta-analysis.Lancet Infect Dis. 2019 Jan;19(1):91-101. doi: 10.1016/S1473-3099(18)30596-6. Lancet Infect Dis. 2019. PMID: 30587297 Free PMC article.
-
Active case detection, treatment of falciparum malaria with combined chloroquine and sulphadoxine/pyrimethamine and vivax malaria with chloroquine and molecular markers of anti-malarial resistance in the Republic of Vanuatu.Malar J. 2010 Apr 6;9:89. doi: 10.1186/1475-2875-9-89. Malar J. 2010. PMID: 20370920 Free PMC article.
-
The risk of Plasmodium vivax parasitaemia after P. falciparum malaria: An individual patient data meta-analysis from the WorldWide Antimalarial Resistance Network.PLoS Med. 2020 Nov 19;17(11):e1003393. doi: 10.1371/journal.pmed.1003393. eCollection 2020 Nov. PLoS Med. 2020. PMID: 33211712 Free PMC article.
Cited by
-
Emerging trends and new developments in global research on artemisinin and its derivatives.Heliyon. 2024 Dec 9;11(1):e41086. doi: 10.1016/j.heliyon.2024.e41086. eCollection 2025 Jan 15. Heliyon. 2024. PMID: 39801992 Free PMC article.
-
Application of a new highly multiplexed amplicon sequencing tool to evaluate Plasmodium falciparum antimalarial resistance and relatedness in individual and pooled samples from Dschang, Cameroon.medRxiv [Preprint]. 2024 Oct 10:2024.10.03.24314715. doi: 10.1101/2024.10.03.24314715. medRxiv. 2024. Update in: Front Parasitol. 2025 Feb 05;3:1509261. doi: 10.3389/fpara.2024.1509261. PMID: 39417120 Free PMC article. Updated. Preprint.
-
Targeting malaria parasites inside mosquitoes: ecoevolutionary consequences.Trends Parasitol. 2022 Dec;38(12):1031-1040. doi: 10.1016/j.pt.2022.09.004. Epub 2022 Oct 5. Trends Parasitol. 2022. PMID: 36209032 Free PMC article. Review.
-
A proposed method of grading malaria chemoprevention efficacy.Trans R Soc Trop Med Hyg. 2023 Nov 3;117(11):761-764. doi: 10.1093/trstmh/trad042. Trans R Soc Trop Med Hyg. 2023. PMID: 37427562 Free PMC article.
-
Antimalarial activity of borrelidin and fumagilin in Plasmodium berghei-infected mice.Open Vet J. 2024 Aug;14(8):2007-2015. doi: 10.5455/OVJ.2024.v14.i8.30. Epub 2024 Aug 31. Open Vet J. 2024. PMID: 39308722 Free PMC article.
References
-
- World Health Organization. Guidelines for malaria. World Health Organisation; Geneva: 2022. https://www.who.int/teams/global-malaria-programme/guidelines-for-malaria .
-
- World Health Organization. Methods for surveillance of antimalarial drugs. 2009. https://www.who.int/docs/default-source/documents/publications/gmp/metho... .
-
- World Health Organization. Guidelines for the Treatment of Malaria. World Health Organization; Geneva: 2015. [accessed 19 February 2022]. https://apps.who.int/iris/bitstream/handle/10665/162441/9789241549127_en... .
-
- White NJ. The assessment of antimalarial drug efficacy. Trends Parasitol. 2002;18:458–464. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
