

Nutritional biomarkers and heart failure requiring hospitalization in patients with type 2 diabetes: the SURDIAGENE cohort
- PMID: 35681209
- PMCID: PMC9185908
- DOI: 10.1186/s12933-022-01505-9
Nutritional biomarkers and heart failure requiring hospitalization in patients with type 2 diabetes: the SURDIAGENE cohort
Abstract
Background: Heart failure (HF) is a growing complication and one of the leading causes of mortality in people living with type 2 diabetes (T2D). Among the possible causes, the excess of red meat and the insufficiency of vegetables consumption are suspected. Such an alimentation is associated with nutritional biomarkers, including trimethylamine N-oxide (TMAO) and its precursors. Here, we aimed to study these biomarkers as potential prognostic factors for HF in patients with T2D.
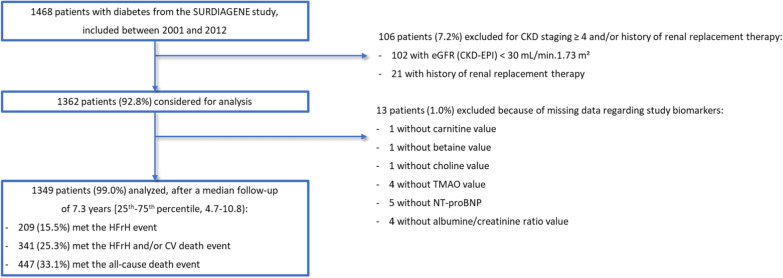
Methods: We used the SURDIAGENE (SURvival DIAbetes and GENEtics) study, a large, prospective, monocentric cohort study including 1468 patients with T2D between 2001 and 2012. TMAO and its precursors (trimethylamine [TMA], betaine, choline, and carnitine) as well as thio-amino-acids (cysteine, homocysteine and methionine) were measured by liquid chromatography-tandem mass spectrometry. The main outcome was HF requiring Hospitalization (HFrH) defined as the first occurrence of acute HF leading to hospitalization and/or death, established by an adjudication committee, based on hospital records until 31st December 2015. The secondary outcomes were the composite event HFrH and/or cardiovascular death and all-cause death. The association between the biomarkers and the outcomes was studied using cause-specific hazard-models, adjusted for age, sex, history of coronary artery disease, NT-proBNP, CKD-EPI-derived eGFR and the urine albumin/creatinine ratio. Hazard-ratios (HR) are expressed for one standard deviation.
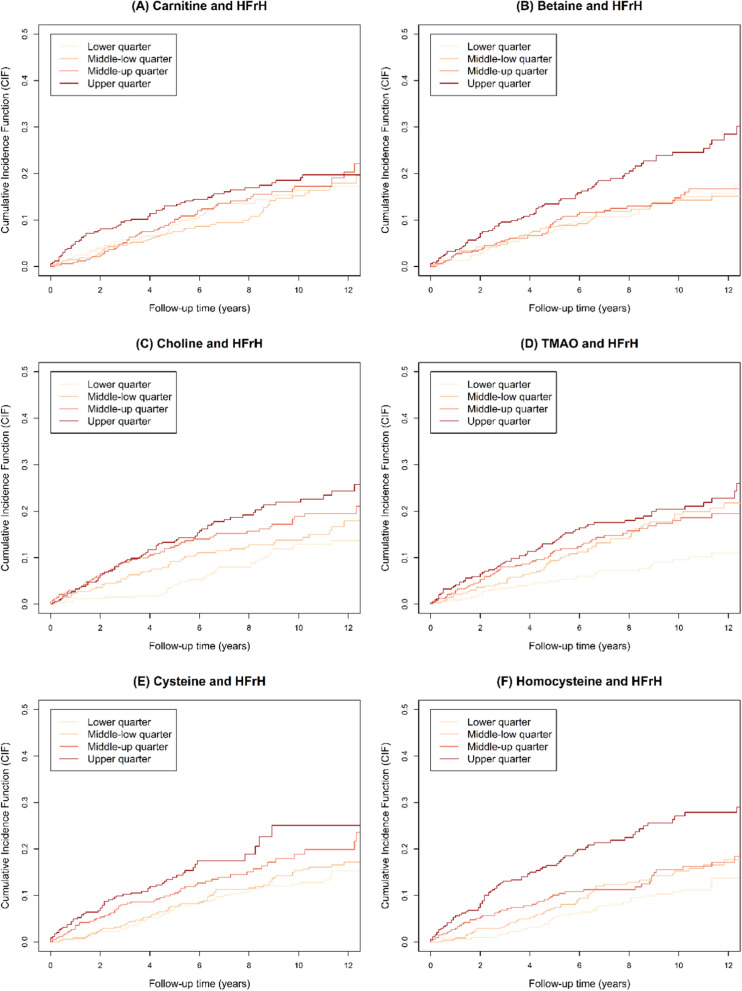
Results: The data of interest were available for 1349/1468 of SURDIAGENE participants (91.9%), including 569 (42.2%) women, with a mean age of 64.3 ± 10.7 years and a median follow-up of 7.3 years [25th-75th percentile, 4.7-10.8]. HFrH was reported in 209 patients (15.5%), HFrH and/or cardiovascular death in 341 (25.3%) and all-cause death in 447 (33.1%). In unadjusted hazard-models, carnitine (HR = 1.20, 95% CI [1.05; 1.37]), betaine (HR = 1.34, [1.20; 1.50]), choline (HR = 1.35, [1.20; 1.52]), TMAO (HR = 1.32, [1.16; 1.50]), cysteine (HR = 1.38, [1.21; 1.58]) and homocysteine (HR = 1.28, [1.17; 1.39]) were associated with HFrH, but not TMA and methionine. In the fully adjusted models, none of these associations was significant, neither for HFrH nor for HFrH and/or CV death, when homocysteine only was positively associated with all-cause death (HR = 1.16, [1.06; 1.27]).
Conclusions: TMAO and its precursors do not appear to be substantial prognosis factors for HFrH, beyond usual cardiac- and kidney-related risk factors, whereas homocysteine is an independent risk factor for all-cause death in patients with T2D.
Keywords: Cohort study; Diabetes mellitus; Heart failure; Homocysteine; Nutritional biomarkers; TMAO.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest related to this work.
Figures
References
-
- IDF Atlas 9th edition and other resources [Internet]. https://diabetesatlas.org/en/resources/. Accessed 30 Apr 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
