

Combination of OX40 Co-Stimulation, Radiotherapy, and PD-1 Inhibition in a Syngeneic Murine Triple-Negative Breast Cancer Model
- PMID: 35681672
- PMCID: PMC9179485
- DOI: 10.3390/cancers14112692
Combination of OX40 Co-Stimulation, Radiotherapy, and PD-1 Inhibition in a Syngeneic Murine Triple-Negative Breast Cancer Model
Abstract
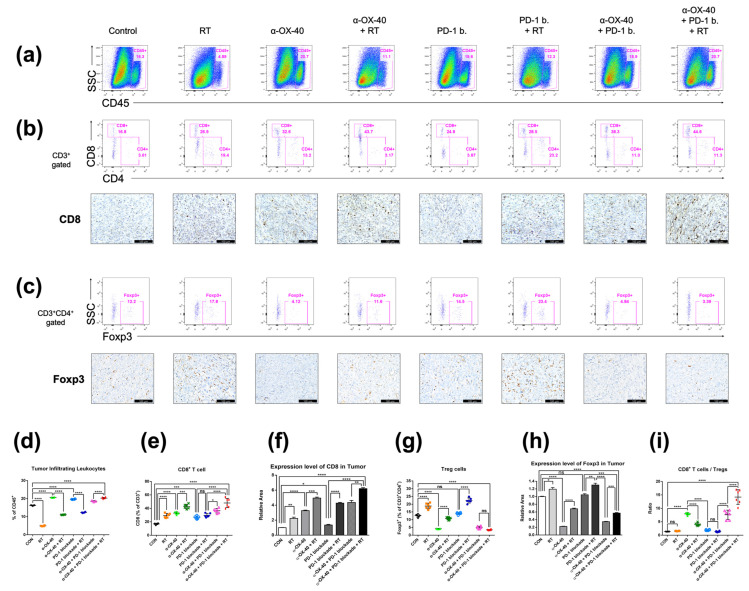
Immune checkpoint inhibitors have been successful in a wide range of tumor types but still have limited efficacy in immunologically cold tumors, such as breast cancers. We hypothesized that the combination of agonistic anti-OX40 (α-OX40) co-stimulation, PD-1 blockade, and radiotherapy would improve the therapeutic efficacy of the immune checkpoint blockade in a syngeneic murine triple-negative breast cancer model. Murine triple-negative breast cancer cells (4T1) were grown in immune-competent BALB/c mice, and tumors were irradiated with 24 Gy in three fractions. PD-1 blockade and α-OX40 were administered five times every other day. Flow cytometric analyses and immunohistochemistry were used to monitor subsequent changes in the immune cell repertoire. The combination of α-OX40, radiotherapy, and PD-1 blockade significantly improved primary tumor control, abscopal effects, and long-term survival beyond 2 months (60%). In the tumor microenvironment, the ratio of CD8+ T cells to CD4 + FOXP3+ regulatory T cells was significantly elevated and exhausted CD8+ T cells (PD-1+, CTLA-4+, TIM-3+, or LAG-3+ cells) were significantly reduced in the triple combination group. Systemically, α-OX40 co-stimulation and radiation significantly increased the CD103+ dendritic cell response in the spleen and plasma IFN-γ, respectively. Together, our results suggest that the combination of α-OX40 co-stimulation and radiation is a viable approach to overcome therapeutic resistance to PD-1 blockade in immunologically cold tumors, such as triple-negative breast cancer.
Keywords: OX40; PD-1; breast cancer; immuno-oncology; immunotherapy; radiotherapy; stereotactic body radiotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
PI3Kαδ Inhibitor Combined With Radiation Enhances the Antitumor Immune Effect of Anti-PD1 in a Syngeneic Murine Triple-Negative Breast Cancer Model.Int J Radiat Oncol Biol Phys. 2021 Jul 1;110(3):845-858. doi: 10.1016/j.ijrobp.2021.01.025. Epub 2021 Feb 26. Int J Radiat Oncol Biol Phys. 2021. PMID: 33642128
-
PI3Kγδ inhibitor plus radiation enhances the antitumour immune effect of PD-1 blockade in syngenic murine breast cancer and humanised patient-derived xenograft model.Eur J Cancer. 2021 Nov;157:450-463. doi: 10.1016/j.ejca.2021.08.029. Epub 2021 Oct 1. Eur J Cancer. 2021. PMID: 34601286
-
PD-1 blockade and OX40 triggering synergistically protects against tumor growth in a murine model of ovarian cancer.PLoS One. 2014 Feb 27;9(2):e89350. doi: 10.1371/journal.pone.0089350. eCollection 2014. PLoS One. 2014. PMID: 24586709 Free PMC article.
-
OX40 Agonists and Combination Immunotherapy: Putting the Pedal to the Metal.Front Oncol. 2015 Feb 16;5:34. doi: 10.3389/fonc.2015.00034. eCollection 2015. Front Oncol. 2015. PMID: 25763356 Free PMC article. Review.
-
OX40 as a novel target for the reversal of immune escape in colorectal cancer.Am J Transl Res. 2021 Mar 15;13(3):923-934. eCollection 2021. Am J Transl Res. 2021. PMID: 33841630 Free PMC article. Review.
Cited by
-
Effects of neoadjuvant stereotactic body radiotherapy plus adebrelimab and chemotherapy for triple-negative breast cancer: A pilot study.Elife. 2023 Dec 22;12:e91737. doi: 10.7554/eLife.91737. Elife. 2023. PMID: 38131294 Free PMC article. Clinical Trial.
-
OX40-OX40L Axis in Cutaneous T-Cell Lymphomas: Pathogenic, Prognostic, and Potential Therapeutic Perspectives.Biomolecules. 2025 May 13;15(5):715. doi: 10.3390/biom15050715. Biomolecules. 2025. PMID: 40427608 Free PMC article. Review.
-
Research hotspots and frontiers of neoadjuvant therapy in triple-negative breast cancer: a bibliometric analysis of publications between 2002 and 2023.Int J Surg. 2024 Aug 1;110(8):4976-4992. doi: 10.1097/JS9.0000000000001586. Int J Surg. 2024. PMID: 39143709 Free PMC article. Review.
-
Modulation of CD8+ T Cell Responses by Radiotherapy-Current Evidence and Rationale for Combination with Immune Checkpoint Inhibitors.Int J Mol Sci. 2023 Nov 24;24(23):16691. doi: 10.3390/ijms242316691. Int J Mol Sci. 2023. PMID: 38069014 Free PMC article. Review.
-
The untapped potential of radiation and immunotherapy for hormone receptor-positive breast cancer.NPJ Breast Cancer. 2025 Jul 24;11(1):77. doi: 10.1038/s41523-025-00796-x. NPJ Breast Cancer. 2025. PMID: 40707495 Free PMC article. Review.
References
-
- Denkert C., von Minckwitz G., Darb-Esfahani S., Lederer B., Heppner B.I., Weber K.E., Budczies J., Huober J., Klauschen F., Furlanetto J., et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19:40–50. doi: 10.1016/S1470-2045(17)30904-X. - DOI - PubMed
-
- Hwang K.T., Kim J., Jung J., Chang J.H., Chai Y.J., Oh S.W., Oh S., Kim Y.A., Park S.B., Hwang K.R. Impact of breast cancer subtypes on prognosis of women with operable invasive breast cancer: A population-based study using SEER database. Clin. Cancer Res. 2019;25:1970–1979. doi: 10.1158/1078-0432.CCR-18-2782. - DOI - PubMed
-
- Loi S., Michiels S., Salgado R., Sirtaine N., Jose V., Fumagalli D., Kellokumpu-Lehtinen P.L., Bono P., Kataja V., Desmedt C., et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: Results from the FinHER trial. Ann. Oncol. 2014;25:1544–1550. doi: 10.1093/annonc/mdu112. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
