

Diagnostic Utility of Bronchoalveolar Lavage in Patients with Acute Leukemia under Broad-Spectrum Anti-Infective Treatment
- PMID: 35681753
- PMCID: PMC9179550
- DOI: 10.3390/cancers14112773
Diagnostic Utility of Bronchoalveolar Lavage in Patients with Acute Leukemia under Broad-Spectrum Anti-Infective Treatment
Abstract
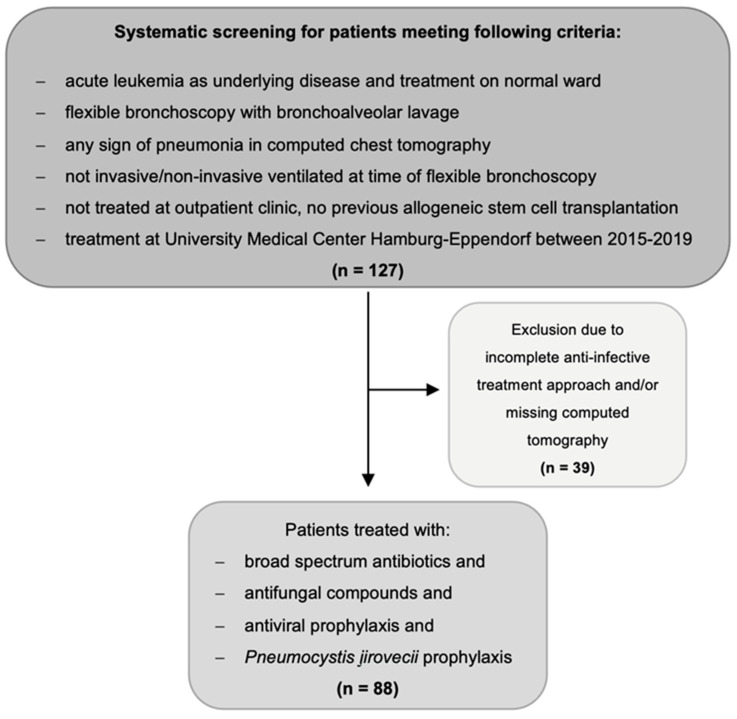
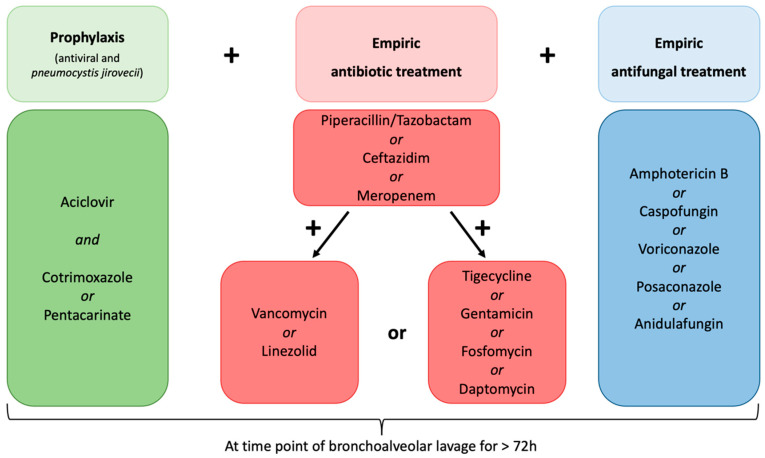
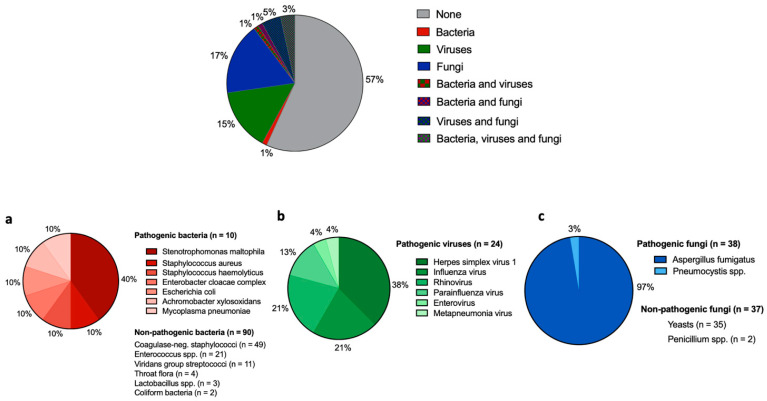
Despite therapeutic advances in the prevention and treatment of febrile neutropenia, acute leukemia (AL) patients still have considerable febrile neutropenia-related mortality. However, the diagnostic yield of flexible bronchoscopy (FB) and bronchoalveolar lavage (BAL) in acute leukemia patients is unclear. In this retrospective single-center study, we analyzed 88 BAL samples of patients with acute leukemia and pulmonary infiltrates in spite of treatment with broad-spectrum anti-infective agents. The aim was to investigate the impact of FB with BAL on detecting causative organisms, which would result in a change in treatment regimens. The median age was 59 years, and 86% had acute myeloid leukemia. In 47%, pathogens were detectable in BAL fluid (pathogen bacteria, viruses, and fungi in 2, 15, and 18%, respectively), with Aspergillus fumigatus detected most frequently. BAL-guided anti-infective therapy changes were performed in 15%. The detection of herpes simplex and influenza viruses were the main reasons for treatment changes. Despite broad-spectrum anti-infective treatment, in approximately half of all patients, pathogens could still be isolated in BAL samples. However, consecutive changes in anti-infective treatment were considerably less frequent, with most changes performed in patients with Herpes simplex virus and Influenza A detection. The need for FB with BAL in patients with AL receiving broad-spectrum empiric anti-infective treatment should therefore be weighed carefully.
Keywords: acute leukemia; bronchoalveolar lavage; flexible bronchoscopy; pneumonia.
Conflict of interest statement
S.G., P.H.v.K., M.S., F.O.H., A.H. and N.B.L. have nothing to declare. H.R. received consulting honoraria from Pfizer, MSD, and Shionogie and received speaker honoraria from Pfizer, MSD, Shinogie, Advanz Pharma, and Infectopharm. C.B. received speaker honoraria from AOK Germany, Bristol Myers Squipp, med update, Merck Serono, Roche Pharma, and Sanofi Aventis; and participated in advisory boards for Astra Zeneca, Bayer Healthcare, Berlin Chemie, Bristol Myers Squipp, GSO Research Organisation, Jansen Cilag, Merck Serono, Merck Sharp Dohme, Novartis, and Sanofi Aventis. W.F. participated in advisory boards for Morphosys, AbbVie, Pfizer, Amgen, Jazz Pharmaceuticals, and Clinigen, received support for meeting attendance from Amgen, Jazz Pharmaceuticals, Daiichi Sankyo Oncology, Bristol-Myers Squibb, and Servier, and received support for medical writing from Amgen, Boehringer Ingelheim, Pfizer, and AbbVie. F.M. received support for meeting attendance from Servier, Abbvie, Incyte, Gilead, Jazz Pharmaceuticals, Novartis, Teva, Pfizer, and Amgen, received support for medical writing from Servier, received research grant from Apis Technologies and Daiichi Sankyo, and received speaker honorarium from Servier, Jazz Pharmaceuticals, and Abbvie.
Figures
References
-
- Taplitz R.A., Kennedy E.B., Bow E.J., Crews J., Gleason C., Hawley D.K., Langston A.A., Nastoupil L.J., Rajotte M., Rolston K.V., et al. Antimicrobial Prophylaxis for Adult Patients with Cancer-Related Immunosuppression: ASCO and IDSA Clinical Practice Guideline Update. J. Clin. Oncol. 2018;36:3043–3054. doi: 10.1200/JCO.18.00374. - DOI - PubMed
LinkOut - more resources
Full Text Sources
