

New Understanding of Diagnosis, Treatment and Prevention of Endometriosis
- PMID: 35682310
- PMCID: PMC9180566
- DOI: 10.3390/ijerph19116725
New Understanding of Diagnosis, Treatment and Prevention of Endometriosis
Abstract
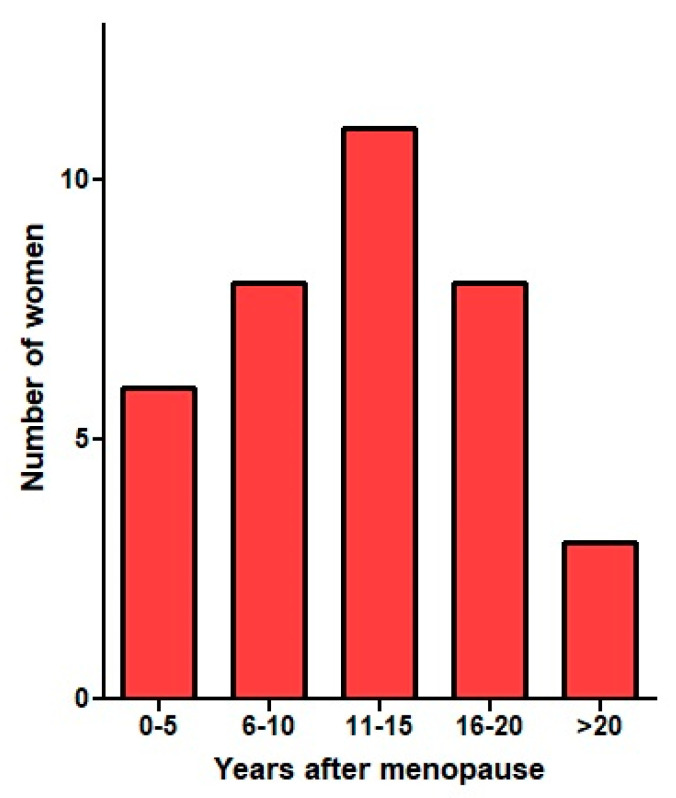
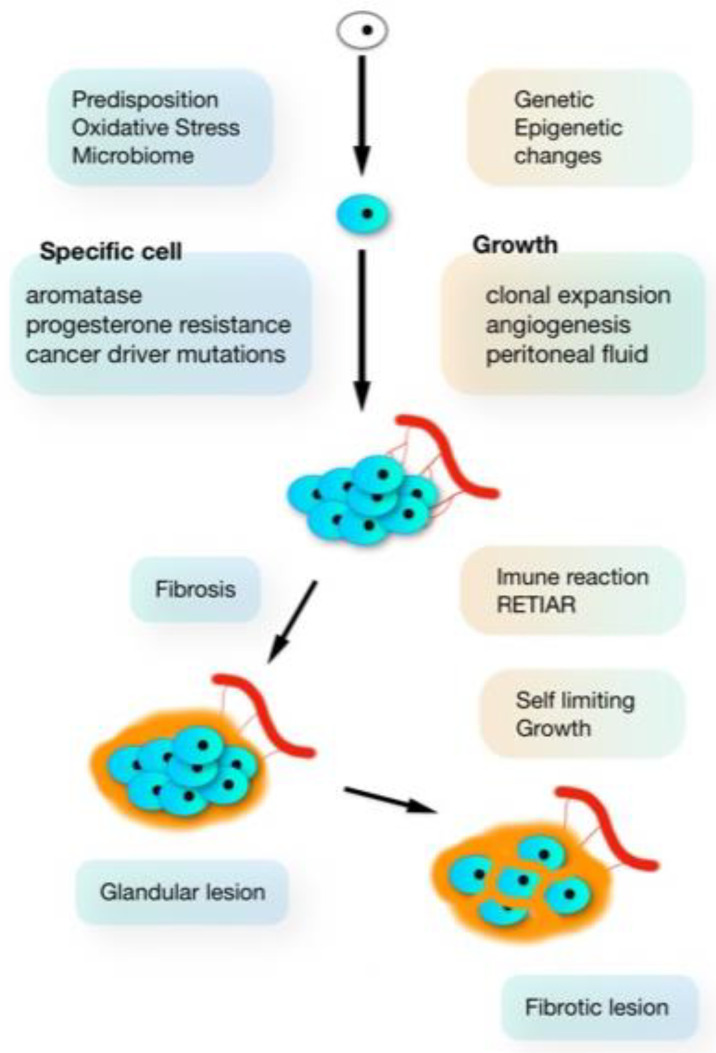
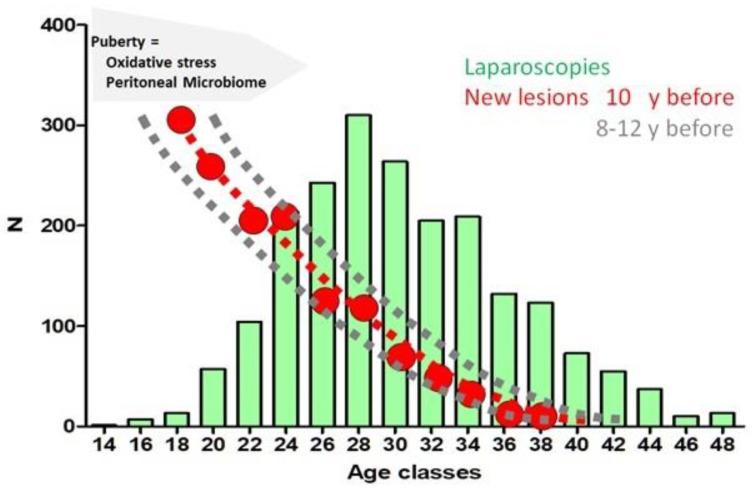
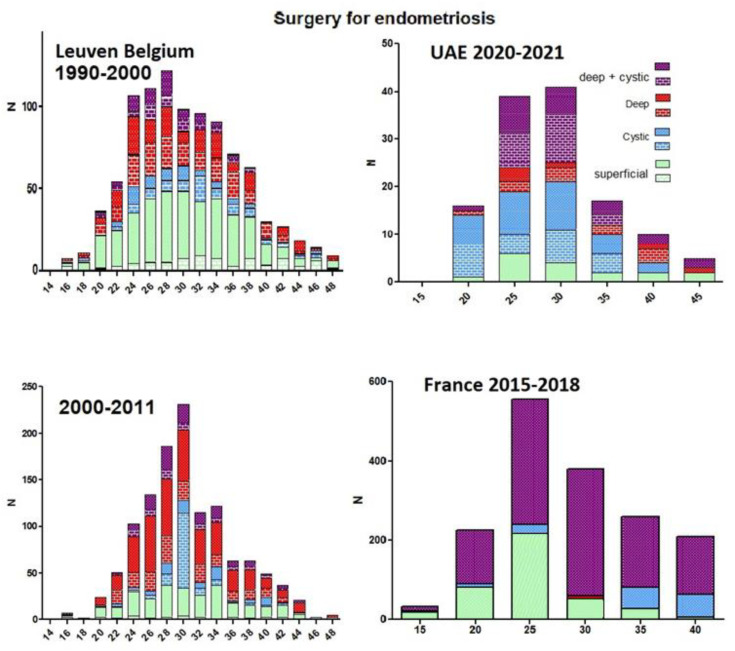
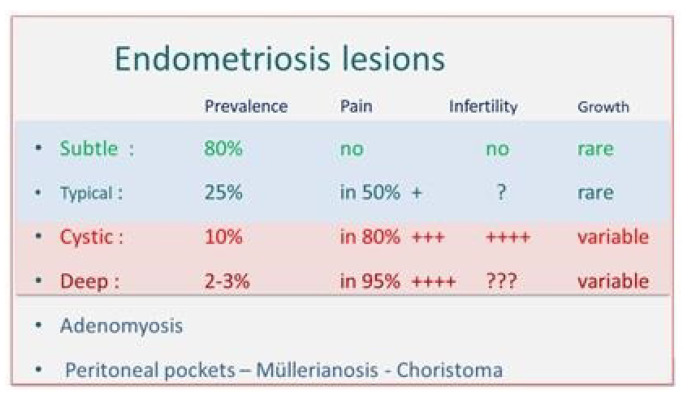
For 100 years, pelvic endometriosis has been considered to originate from the implantation of endometrial cells following retrograde menstruation or metaplasia. Since some observations, such as the clonal aspect, the biochemical variability of lesions and endometriosis in women without endometrium, the genetic-epigenetic (G-E) theory describes that endometriosis only begins after a series of cumulative G-E cellular changes. This explains that the endometriotic may originate from any pluripotent cell apart from the endometrium, that 'endometrium-like cells' can harbour important G-E differences, and that the risk is higher in predisposed women with more inherited incidents. A consequence is a high risk after puberty which decreases progressively thereafter. Considering a 10-year delay between initiation and performing a laparoscopy, this was observed in the United Arab Emirates, Belgium, France and USA. The subsequent growth varies with the G-E changes and the environment but is self-limiting probably because of the immunologic reaction and fibrosis. That each lesion has a different set of G-E incidents explains the variability of pain and the response to hormonal treatment. New lesions may develop, but recurrences after surgical excision are rare. The fibrosis around endometriosis belongs to the body and does not need to be removed. This suggests conservative excision or minimal bowel without safety margins and superficial treatment of ovarian endometriosis. This G-E concept also suggests prevention by decreasing oxidative stress from retrograde menstruation or the peritoneal microbiome. This suggests the prevention of vaginal infections and changes in the gastrointestinal microbiota through food intake and exercise. In conclusion, a higher risk of initiating endometriosis during adolescence was observed in UAE, France, Belgium and USA. This new understanding and the limited growth opens perspectives for earlier diagnosis and better treatment.
Keywords: adenomyoisis; endeometriosis; genetic and epgigenetic; medical therapy; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Pathogenesis Based Diagnosis and Treatment of Endometriosis.Front Endocrinol (Lausanne). 2021 Nov 25;12:745548. doi: 10.3389/fendo.2021.745548. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34899597 Free PMC article. Review.
-
Abnormally located SSEA1+/SOX9+ endometrial epithelial cells with a basalis-like phenotype in the eutopic functionalis layer may play a role in the pathogenesis of endometriosis.Hum Reprod. 2019 Jan 1;34(1):56-68. doi: 10.1093/humrep/dey336. Hum Reprod. 2019. PMID: 30496412 Free PMC article.
-
Pathogenesis of endometriosis: the genetic/epigenetic theory.Fertil Steril. 2019 Feb;111(2):327-340. doi: 10.1016/j.fertnstert.2018.10.013. Epub 2018 Dec 7. Fertil Steril. 2019. PMID: 30527836 Review.
-
The Antigen-Processing Pathway via Major Histocompatibility Complex I as a New Perspective in the Diagnosis and Treatment of Endometriosis.Arch Immunol Ther Exp (Warsz). 2024 Mar 13;72(1). doi: 10.2478/aite-2024-0008. eCollection 2024 Jan 1. Arch Immunol Ther Exp (Warsz). 2024. PMID: 38478380 Review.
-
Endometriosis: Classification, pathophysiology, and treatment options.Pathol Res Pract. 2023 Nov;251:154847. doi: 10.1016/j.prp.2023.154847. Epub 2023 Oct 4. Pathol Res Pract. 2023. PMID: 37844487 Review.
Cited by
-
Shared Pathogenic and Therapeutic Characteristics of Endometriosis, Adenomyosis, and Endometrial Cancer: A Comprehensive Literature Review.Pharmaceuticals (Basel). 2024 Feb 28;17(3):311. doi: 10.3390/ph17030311. Pharmaceuticals (Basel). 2024. PMID: 38543097 Free PMC article. Review.
-
Colonic endometriosis: from subtotal bowel obstruction to malignant transformation - a case series and literature review.World J Surg Oncol. 2025 Jun 11;23(1):230. doi: 10.1186/s12957-025-03888-x. World J Surg Oncol. 2025. PMID: 40500693 Free PMC article. Review.
-
Logistic regression analysis of pregnancy outcome and EFI score of infertile patients with ovarian endometriosis cyst after staged oral administration of traditional Chinese medicine.Front Endocrinol (Lausanne). 2025 Jul 4;16:1624925. doi: 10.3389/fendo.2025.1624925. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40687588 Free PMC article.
-
Gut and reproductive tract microbiota: Insights into the pathogenesis of endometriosis (Review).Biomed Rep. 2023 May 29;19(1):43. doi: 10.3892/br.2023.1626. eCollection 2023 Jul. Biomed Rep. 2023. PMID: 37324168 Free PMC article. Review.
-
Superficial Endometriosis at Ultrasound Examination-A Diagnostic Criteria Proposal.Diagnostics (Basel). 2023 May 27;13(11):1876. doi: 10.3390/diagnostics13111876. Diagnostics (Basel). 2023. PMID: 37296728 Free PMC article.
References
-
- Sampson J.A. Perforating hemorrhagic (chocolate) cysts of the ovary. Their importance and especially their relation to pelvic adenomas of the endometrial type. Arch. Surg. 1921;3:245–323. doi: 10.1001/archsurg.1921.01110080003001. - DOI
-
- Cullen T.S. Adeno-myoma uteri diffusum benignum. Johns Hopkins Hosp. Rep. 1897;6:133–157.
-
- Kempers R.D., Dockerty M.B., Hunt A.B., Symmonds R.E. Significant postmenopausal endometriosis. Surg. Gynecol. Obstet. 1960;111:348–356. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
