

Inverted Papilloma of the Maxillary Sinus: A Recurrence Analysis According to Surgical Approaches
- PMID: 35683409
- PMCID: PMC9181515
- DOI: 10.3390/jcm11113020
Inverted Papilloma of the Maxillary Sinus: A Recurrence Analysis According to Surgical Approaches
Abstract
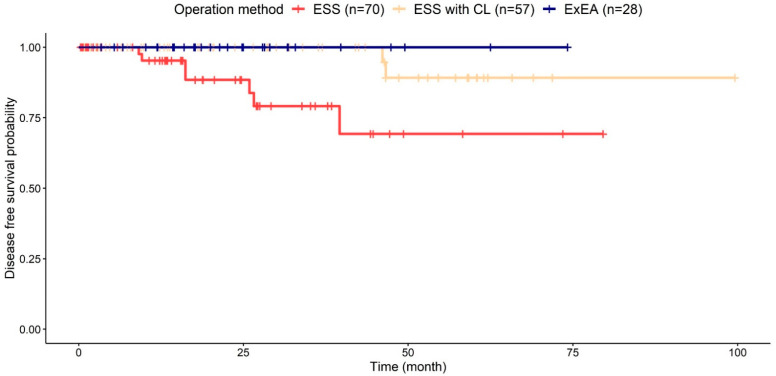
(1) Background: Various surgical approaches have been introduced to resect inverted papillomas (IP) stemming from the maxillary sinus (MS). This study aimed to compare the recurrence rates of IPs originating from the MS according to various surgical modalities. (2) Methods: A total of 155 surgical cases of sinonasal IPs originating from the MS were categorized into three groups according to the surgical approach adopted: endoscopic resection via middle or inferior meatus antrostomy (ESS), ESS with Caldwell−Luc approach or canine fossa trephination (ESS with CL), and expanded endoscopic approaches (ExEA) including endoscopic medial maxillectomy or a prelacrimal recess approach. A Kaplan−Meier curve was generated to examine the recurrence rates. (3) Results: The overall recurrence rate was 5.8% (9/155) with a mean follow-up period of 24.2 months. The recurrence rates for the ESS, ESS with CL, and ExEA groups were 10.0% (7/70), 3.5% (2/57), and 0% (0/28), respectively. The ExEA group had a significantly lower recurrence rate than the ESS group (p = 0.024) and there was a tendency for lower recurrence compared to the ESS within the CL group (p = 0.145). The ExEA required a shorter postoperative hospitalization period than in ESS with CL (p < 0.001). (4) Conclusions: ExEAs to the maxillary sinus such as the PLR and EMM approaches are excellent surgical options for IPs originating from the MS.
Keywords: inverted; maxillary sinus; papilloma; paranasal sinuses.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Lund V.J., Stammberger H., Nicolai P., Castelnuovo P., Beal T., Beham A., Bernal-Sprekelsen M., Braun H., Cappabianca P., Carrau R., et al. European position paper on endoscopic management of tumours of the nose, paranasal sinuses and skull base. Rhinology. 2010;22:1–143. - PubMed
LinkOut - more resources
Full Text Sources
