

Flow Diversion for the Management of Ruptured Intracranial Arterial Infudibular Dilatation: Proof of Principle and Therapeutic Protocol
- PMID: 35685737
- PMCID: PMC9170923
- DOI: 10.3389/fneur.2022.913879
Flow Diversion for the Management of Ruptured Intracranial Arterial Infudibular Dilatation: Proof of Principle and Therapeutic Protocol
Abstract
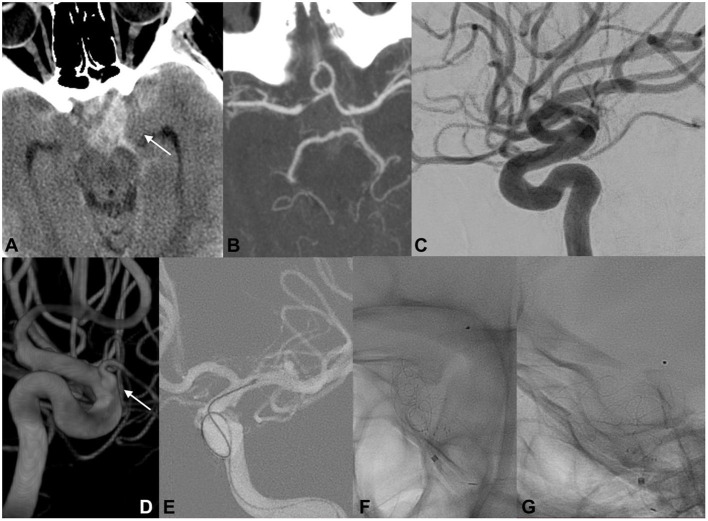
Thought to be benign anatomical variants, cerebral infundibular dilatations (ID) are most commonly encountered at the junction of the internal carotid artery (ICA) and the posterior communicating artery (PcomA). The true nature of this entity remains controversial, as some literature reports suggest they should be considered preaneurysmal lesions and a potential source of devastating subarachnoid hemorrhage. This report describes cases of presumably ruptured IDs and their therapeutic endovascular management. We retrospectively reviewed and analyzed patients with isolated subarachnoid hemorrhage (SAH) where the only potential cause was ruptured cerebral IDs, treated or not, between January 2012 and June 2021. Morphological and radiological features, treatment and procedural considerations, clinical and angiographic outcomes were also reviewed. Natural history of the ID is poorly understood, and its relation to SAH remains controversial. Ruptured cerebral IDs can be the suspected cause of bleeding if no other vascular lesion is present during multimodal examinations. Endovascular flow diversion stenting is safe and effective for the proper treatment of ruptured IDs. Pending further validations with longitudinal data are needed to legitimate the natural course of these mysterious lesions.
Keywords: anterior choroidal artery; flow diverter; infundibular dilatation; posterior communicating arteries; subarachnoid hemorrhage.
Copyright © 2022 Matanov, Sirakova, Chupetlovksa, Penkov, Monov, Krupev, Minkin, Ninov, Karakostov and Sirakov.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Ruptured Infundibular dilatation of the posterior communicating artery.Acta Neurochir (Wien). 2021 Mar;163(3):797-803. doi: 10.1007/s00701-021-04716-3. Epub 2021 Feb 1. Acta Neurochir (Wien). 2021. PMID: 33527210
-
Stability of infundibular dilatations: a single center follow-up study and systematic review of the literature.Acta Neurochir (Wien). 2024 Jan 30;166(1):48. doi: 10.1007/s00701-024-05890-w. Acta Neurochir (Wien). 2024. PMID: 38286939 Free PMC article.
-
Treatment of Ruptured Anterior Choroidal Artery Aneurysms by Acute Coiling Followed by Flow Diversion.World Neurosurg. 2023 Aug;176:e162-e172. doi: 10.1016/j.wneu.2023.05.023. Epub 2023 May 12. World Neurosurg. 2023. PMID: 37178914
-
Are infundibular dilatations at risk of further transformation? Ten-year progression of a prior documented infundibulum into a saccular aneurysm and rupture: Case report and a review of the literature.Neurochirurgie. 2014 Dec;60(6):307-11. doi: 10.1016/j.neuchi.2014.04.001. Epub 2014 Sep 16. Neurochirurgie. 2014. PMID: 25239381 Review.
-
[Ruptured internal carotid -posterior communicating artery aneurysm associated with an anomalous hyperplastic anterior choroidal artery and aneurysm: case report].No Shinkei Geka. 2005 Feb;33(2):155-62. No Shinkei Geka. 2005. PMID: 15714961 Review. Japanese.
References
-
- Pool JL, Potts DG. Aneurysms and Arteriovenous Anomalies of the Brain : Diagnosis and Treatment. New York, NY: Harper & Row; (1965).
-
- Taveras JM, Wood EH. Diagnostic Neuroradiology. 2d ed. Baltimore, MD: Williams & Wilkins Co. (1976).
-
- Kim HS, Kim EJ, Lee KM, Choi WS. Aneurysm and infundibular dilatation at an unusual origin of the ophthalmic artery. J Korean Soc Radiol. (2014) 71:164. 10.3348/jksr.2014.71.4.164 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous