

Patient-specific Implants for Treating Atrophic Mandibles
- PMID: 35685746
- PMCID: PMC9170002
- DOI: 10.1097/GOX.0000000000004359
Patient-specific Implants for Treating Atrophic Mandibles
Abstract
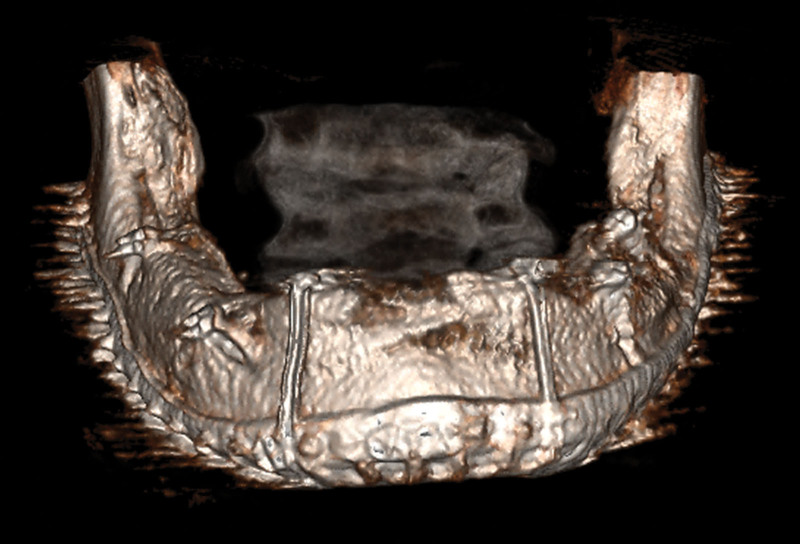
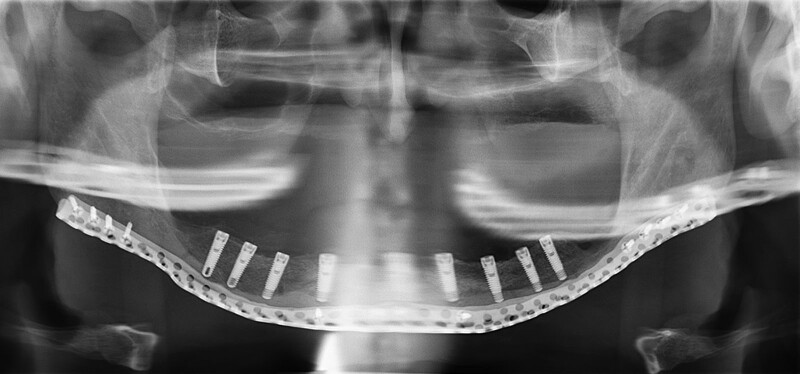
Extremely atrophic mandibles are difficult to treat. Most patients choose to live with removable dentures. However, what if the atrophy is so extreme that spontaneous fractures occur? The objective of this report is to offer a single-stage augmentation method, which uses patient-specific crib-shaped implants (PSI) combined with autogenous free bone grafts. PSI were planned using three-dimensional (3D) segmentation and 3D virtual-planning software. Implants were designed according to the patient's mandible with a mesh-like structure and included large holes for allowing blood supply recovery. During surgery, the PSI fitted perfectly. In cases exhibiting malposition of the mandibular fragments, repositioning was performed using 3D virtual planning. When repositioning mandibular segments, the PSI served as a guide for the correct positioning. Iliac-crest bone graft was harvested and fixed as an onlay over the residual mandibular basal bone. External approach was used to avoid contamination. Six months following surgery, fixation wires were removed, and dental implants were positioned in the newly formed bone. The PSI allowed for rigid fixation, thus leading to optimal incorporation of the iliac-crest bone graft. No further augmentation was required. Bony continuity for future stability and secession of the spontaneous fractures was achieved. Dental implants were placed effortlessly. Treating extremely atrophic mandibles is an entity of its own and is considered one of the most challenging in craniofacial reconstruction. It mostly requires multiple operations with high rates of failure. We offer a novel method of 3D mandibular reconstruction, both vertically and horizontally, showing promising results and achieving enough bone for further dental rehabilitation.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Figures


References
-
- Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971;26:266–279. - PubMed
-
- Frost HM. Bone’s mechanostat: a 2003 update. Anat Rec A Discov Mol Cell Evol Biol. 2003;275:1081–1101. - PubMed
-
- Bras J. Mandibular atrophy and metabolic bone loss. Int Dent J. 1990;40:298–302. - PubMed
-
- Denissen HW, Kalk W, Veldhuis HA, et al. . Anatomic considerations for preventive implantation. Int J Oral Maxillofac Implants. 1993;8:191–196. - PubMed
-
- Cope MR. Spontaneous fracture of an atrophic endentulous mandible treated without fixation. Br J Oral Surg. 1982;20:22–30. - PubMed
LinkOut - more resources
Full Text Sources