

Incidence, Attributable Mortality, and Healthcare and Out-of-Pocket Costs of Clostridioides difficile Infection in US Medicare Advantage Enrollees
- PMID: 35686435
- PMCID: PMC9907506
- DOI: 10.1093/cid/ciac467
Incidence, Attributable Mortality, and Healthcare and Out-of-Pocket Costs of Clostridioides difficile Infection in US Medicare Advantage Enrollees
Abstract
Background: US attributable Clostridioides difficile infection (CDI) mortality and cost data are primarily from Medicare fee-for-service populations, and little is known about Medicare Advantage Enrollees (MAEs). This study evaluated CDI incidence among MAEs from 2012 to 2019 and determined attributable mortality and costs by comparing MAEs with and without CDI occurring in 2018.
Methods: This retrospective cohort study assessed CDI incidence and associated mortality and costs for eligible MAEs ≥65 years of age using the de-identified Optum Clinformatics Data Mart database (Optum; Eden Prairie, Minnesota, USA). Outcomes included mortality, healthcare utilization, and costs, which were assessed via a propensity score-matched cohort using 2018 as the index year. Outcome analyses were stratified by infection acquisition and hospitalization status.
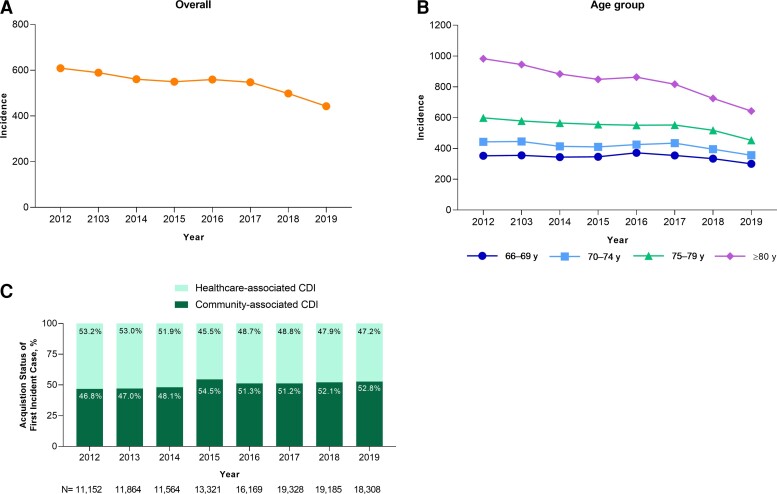
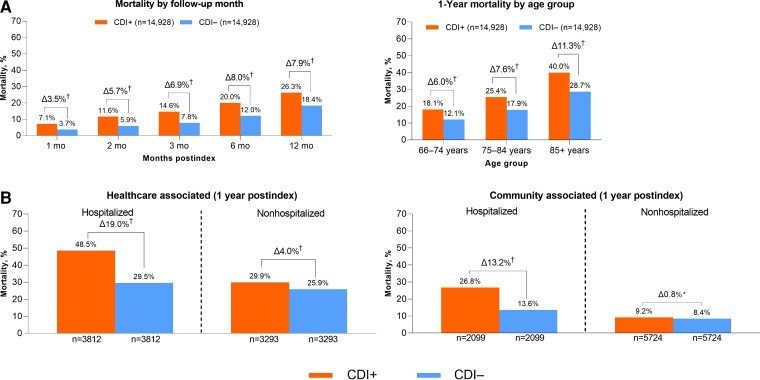
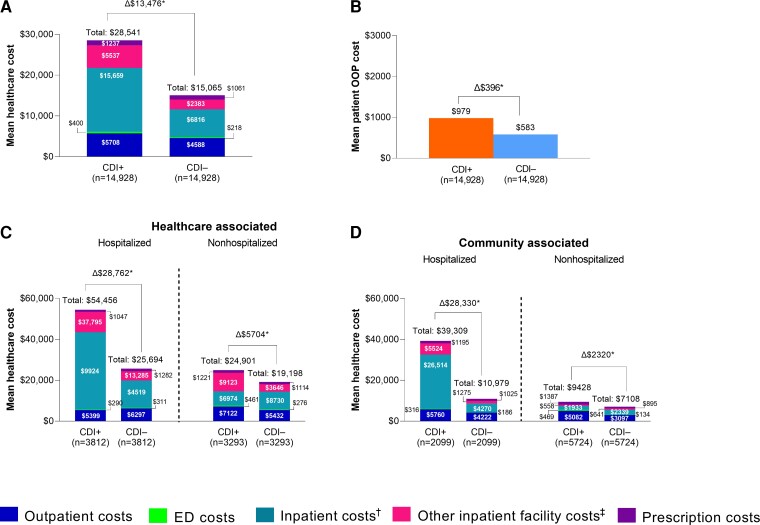
Results: From 2012 to 2019, overall annual CDI incidence declined from 609 to 442 per 100 000 person-years. Although the incidence of healthcare-associated CDI declined overall (2012, 53.2%; 2019, 47.2%), community-associated CDI increased (2012, 46.8%; 2019, 52.8%). The 1-year attributable mortality was 7.9% (CDI cases, 26.3%; non-CDI controls, 18.4%). At the 2-month follow-up, CDI-associated excess mean total healthcare and out-of-pocket costs were $13 476 and $396, respectively. Total excess mean healthcare costs were greater among hospitalized (healthcare-associated, $28 762; community-associated, $28 330) than nonhospitalized CDI patients ($5704 and $2320, respectively), whereas total excess mean out-of-pocket cost was highest among community-associated hospitalized CDI patients ($970).
Conclusions: CDI represents an important public health burden in the MAE population. Preventive strategies and treatments are needed to improve outcomes and reduce costs for healthcare systems and this growing population of older US adults.
Keywords: Clostridioides difficile; Medicare Advantage; costs; incidence; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. H. Y., T. A., J. L. N., and J. Z. are employees of Pfizer Inc, and may hold stock or stock options, and Pfizer pays for conference attendance. M. A. O. reports grant funding and consulting work funded by Pfizer Inc. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med 2015; 372:1539–48. - PubMed
-
- Kelly CP, Pothoulakis C, LaMont JT. Clostridium difficile colitis. N Engl J Med 1994; 330:257–62. - PubMed
-
- Keller JM, Surawicz CM. Clostridium difficile infection in the elderly. Clin Geriatr Med 2014; 30:79–93. - PubMed
-
- Simor AE, Bradley SF, Strausbaugh LJ, Crossley K, Nicolle LE; SHEA Long-Term-Care Committee. Clostridium difficile in long-term-care facilities for the elderly. Infect Control Hosp Epidemiol 2002; 23:696–703. - PubMed
-
- Kim JH, Toy D, Muder RR. Clostridium difficile infection in a long-term care facility: hospital-associated illness compared with long-term care-associated illness. Infect Control Hosp Epidemiol 2011; 32:656–60. - PubMed
