

Subtyping of common complex diseases and disorders by integrating heterogeneous data. Identifying clusters among women with lower urinary tract symptoms in the LURN study
- PMID: 35687541
- PMCID: PMC9187122
- DOI: 10.1371/journal.pone.0268547
Subtyping of common complex diseases and disorders by integrating heterogeneous data. Identifying clusters among women with lower urinary tract symptoms in the LURN study
Abstract
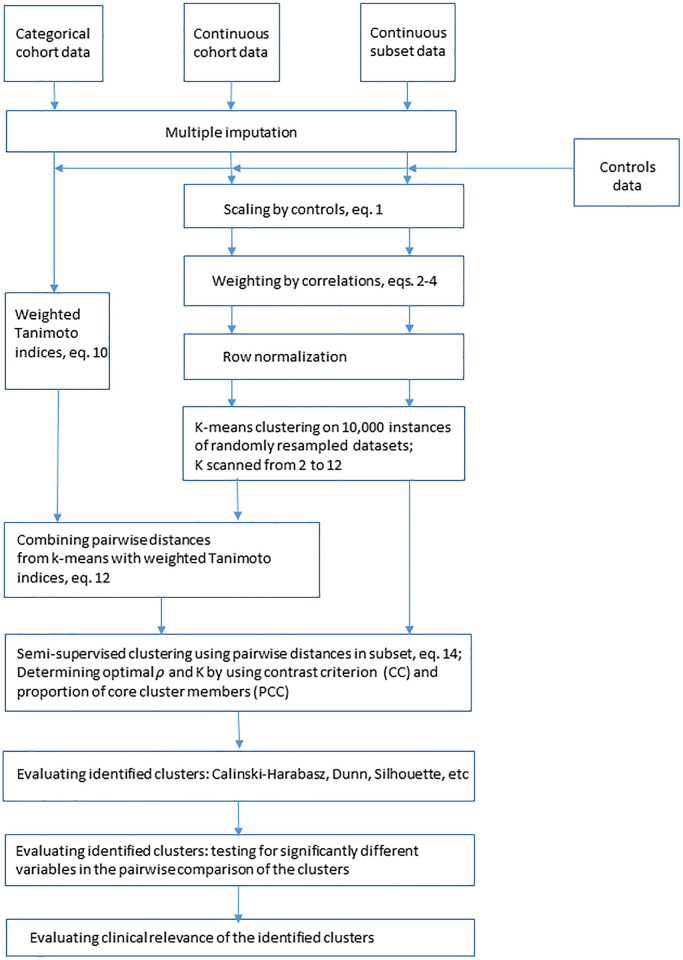
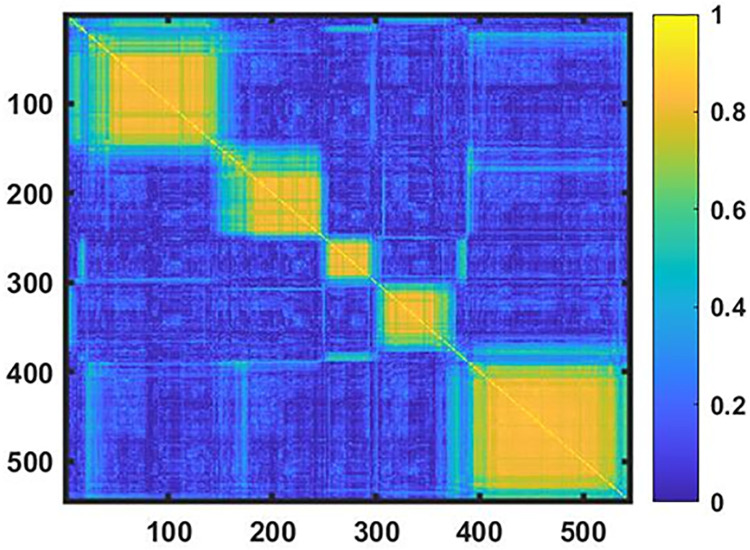
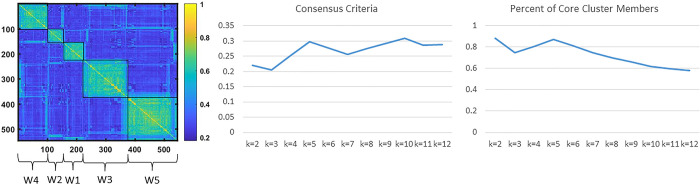
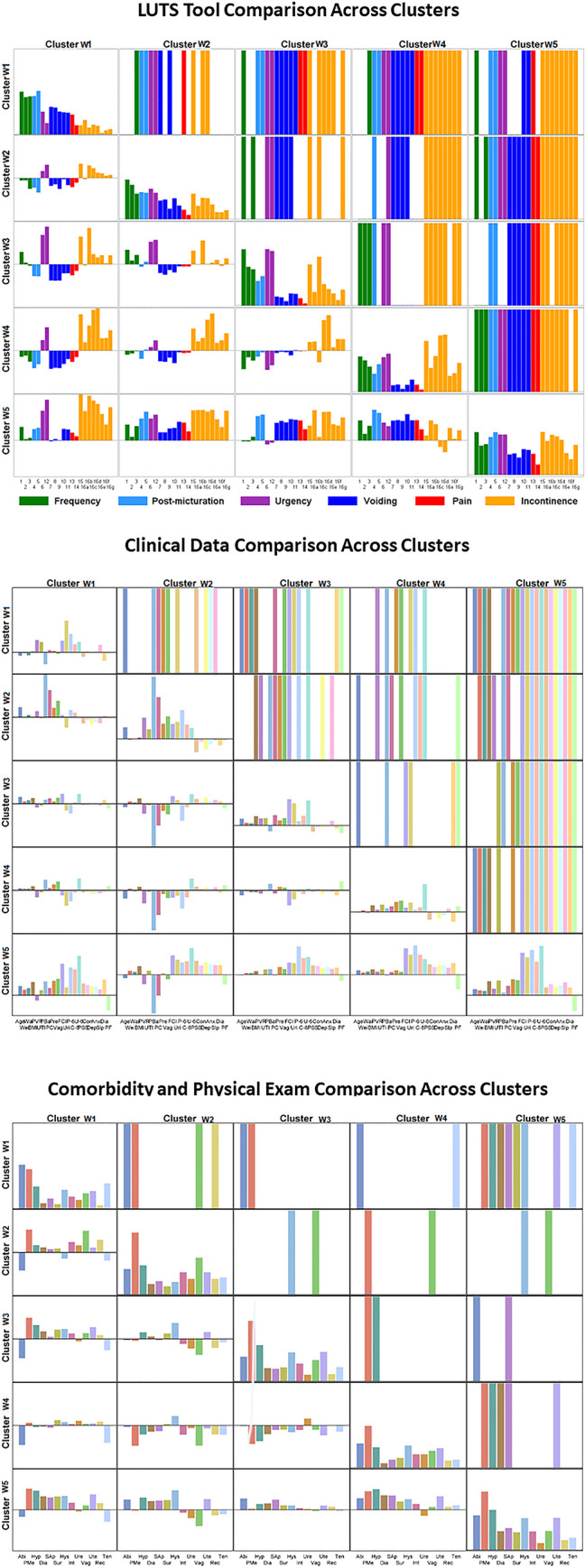
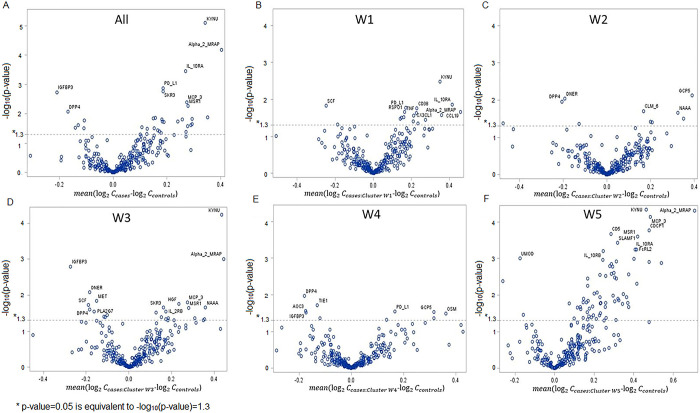
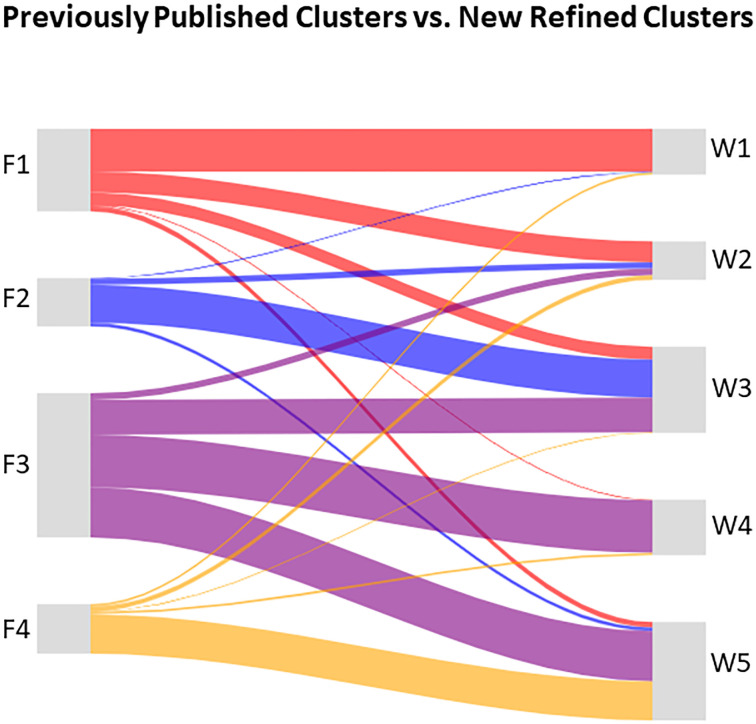
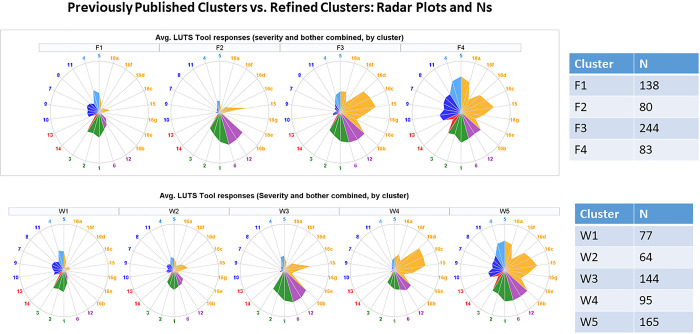
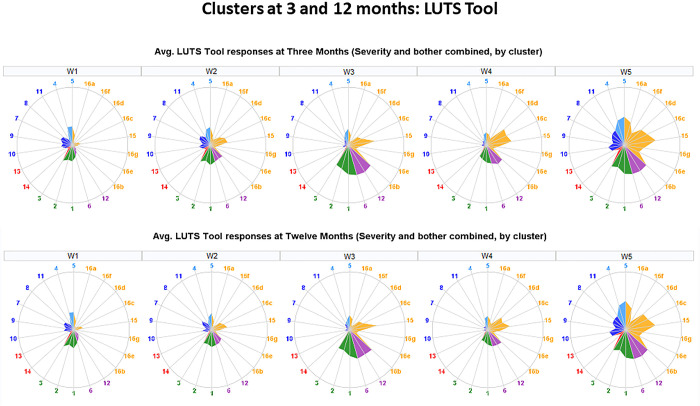
We present a methodology for subtyping of persons with a common clinical symptom complex by integrating heterogeneous continuous and categorical data. We illustrate it by clustering women with lower urinary tract symptoms (LUTS), who represent a heterogeneous cohort with overlapping symptoms and multifactorial etiology. Data collected in the Symptoms of Lower Urinary Tract Dysfunction Research Network (LURN), a multi-center observational study, included self-reported urinary and non-urinary symptoms, bladder diaries, and physical examination data for 545 women. Heterogeneity in these multidimensional data required thorough and non-trivial preprocessing, including scaling by controls and weighting to mitigate data redundancy, while the various data types (continuous and categorical) required novel methodology using a weighted Tanimoto indices approach. Data domains only available on a subset of the cohort were integrated using a semi-supervised clustering approach. Novel contrast criterion for determination of the optimal number of clusters in consensus clustering was introduced and compared with existing criteria. Distinctiveness of the clusters was confirmed by using multiple criteria for cluster quality, and by testing for significantly different variables in pairwise comparisons of the clusters. Cluster dynamics were explored by analyzing longitudinal data at 3- and 12-month follow-up. Five clusters of women with LUTS were identified using the developed methodology. None of the clusters could be characterized by a single symptom, but rather by a distinct combination of symptoms with various levels of severity. Targeted proteomics of serum samples demonstrated that differentially abundant proteins and affected pathways are different across the clusters. The clinical relevance of the identified clusters is discussed and compared with the current conventional approaches to the evaluation of LUTS patients. The rationale and thought process are described for the selection of procedures for data preprocessing, clustering, and cluster evaluation. Suggestions are provided for minimum reporting requirements in publications utilizing clustering methodology with multiple heterogeneous data domains.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Irwin DE, Milsom I, Hunskaar S, Reilly K, Kopp Z, Herschorn S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306–1314; discussion 1314–1305. doi: 10.1016/j.eururo.2006.09.019 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
