

Development of protective equipment for endoscopic treatment and surgery in otorhinolaryngology
- PMID: 35687567
- PMCID: PMC9187069
- DOI: 10.1371/journal.pone.0268974
Development of protective equipment for endoscopic treatment and surgery in otorhinolaryngology
Abstract
Objective: The coronavirus disease pandemic has raised concerns regarding the transmission of infections to healthcare workers. We developed a new protective device to reduce the risk of aerosol diffusion and droplet infection among healthcare workers. Here, we report the results of a theoretical evaluation of the efficacy of this device.
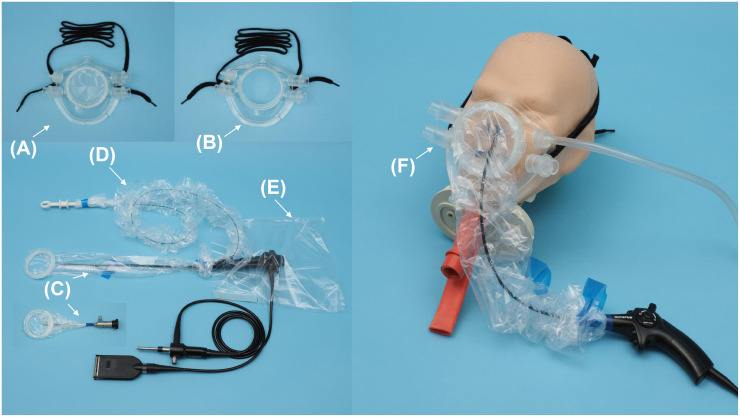
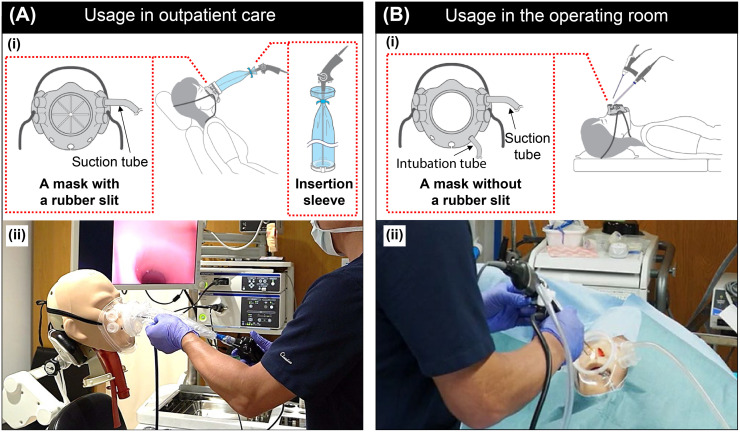
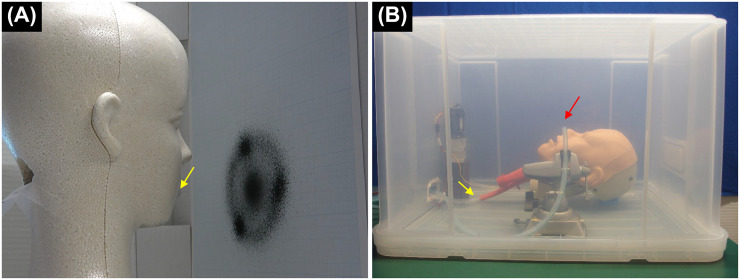
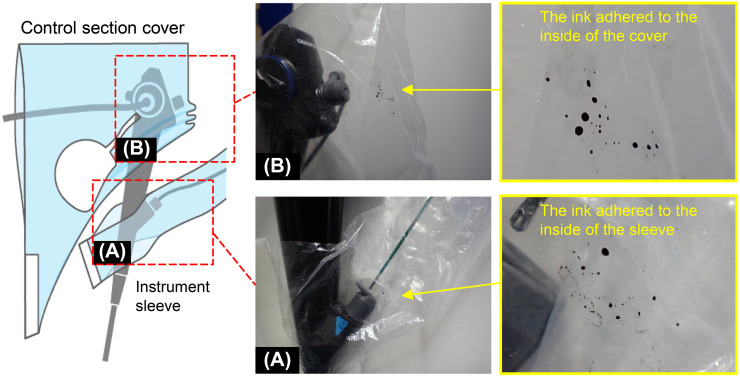
Methods: We used suction-capable masks with and without rubber slits, sleeves for the insertion section of endoscopes and treatment tools, and a cover for the control section of the endoscope. To simulate droplet spread from patients, we created a droplet simulation model and an aerosol simulation model. The results with and without the devices attached and with and without the suction were compared.
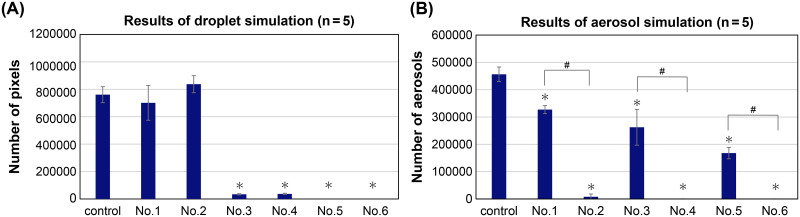
Results: The droplet simulation model showed a 95% reduction in droplets with masks with rubber slits; furthermore, a reduction of 100% was observed when the insertion sleeve was used. Evaluation of aerosol simulation when suction was applied revealed an aerosol reduction of 98% and >99% with the use of the mask without rubber slits and with the combined use of the mask and insertion sleeve, respectively. The elimination of droplet emission upon instrument removal confirmed that the instrument sleeve prevented the diffusion of droplets. The elimination of droplets upon repeated pressing of the suction button confirmed that the cover prevented the diffusion of droplets.
Conclusion: We developed a device for infection control, in collaboration with a gastrointestinal endoscopist and Olympus Medical Systems Corporation, that was effective in reducing droplet and aerosol diffusion in this initial theoretical assessment.
Conflict of interest statement
This research and development endeavor was conducted in collaboration with Olympus Medical Systems Corporation and a gastrointestinal endoscopist (Dr. Daisuke Kikuchi). Matsuwaki Clinic Shinagawa and Olympus Medical Systems Corporation have concluded an advisory agreement regarding this development. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Droplet and Aerosol Generation With Endonasal Surgery: Methods to Mitigate Risk During the COVID-19 Pandemic.Otolaryngol Head Neck Surg. 2021 Feb;164(2):285-293. doi: 10.1177/0194599820949802. Epub 2020 Aug 11. Otolaryngol Head Neck Surg. 2021. PMID: 32779964 Free PMC article.
-
Design and quantitative evaluation of 'Aerosol Bio-Containment Device (ABCD)' for reducing aerosol exposure during infectious aerosol-generating events.PLoS One. 2023 Jan 6;18(1):e0272716. doi: 10.1371/journal.pone.0272716. eCollection 2023. PLoS One. 2023. PMID: 36608021 Free PMC article.
-
A novel mask to prevent aerosolized droplet dispersion in endoscopic procedures during the coronavirus disease pandemic.Medicine (Baltimore). 2021 Jul 2;100(26):e26048. doi: 10.1097/MD.0000000000026048. Medicine (Baltimore). 2021. PMID: 34190142 Free PMC article.
-
Guidance for otolaryngology health care workers performing aerosol generating medical procedures during the COVID-19 pandemic.J Otolaryngol Head Neck Surg. 2020 Jun 3;49(1):36. doi: 10.1186/s40463-020-00429-2. J Otolaryngol Head Neck Surg. 2020. PMID: 32493489 Free PMC article. Review.
-
Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review.Anaesthesia. 2020 Aug;75(8):1086-1095. doi: 10.1111/anae.15093. Epub 2020 May 8. Anaesthesia. 2020. PMID: 32311771 Free PMC article. Review.
Cited by
-
Shielding device for endoscopic procedures during lower gastrointestinal endoscopy.DEN Open. 2022 Oct 10;3(1):e173. doi: 10.1002/deo2.173. eCollection 2023 Apr. DEN Open. 2022. PMID: 36247315 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
