

Fetal cardiovascular blood flow MRI: techniques and applications
- PMID: 35687661
- PMCID: PMC10321246
- DOI: 10.1259/bjr.20211096
Fetal cardiovascular blood flow MRI: techniques and applications
Abstract
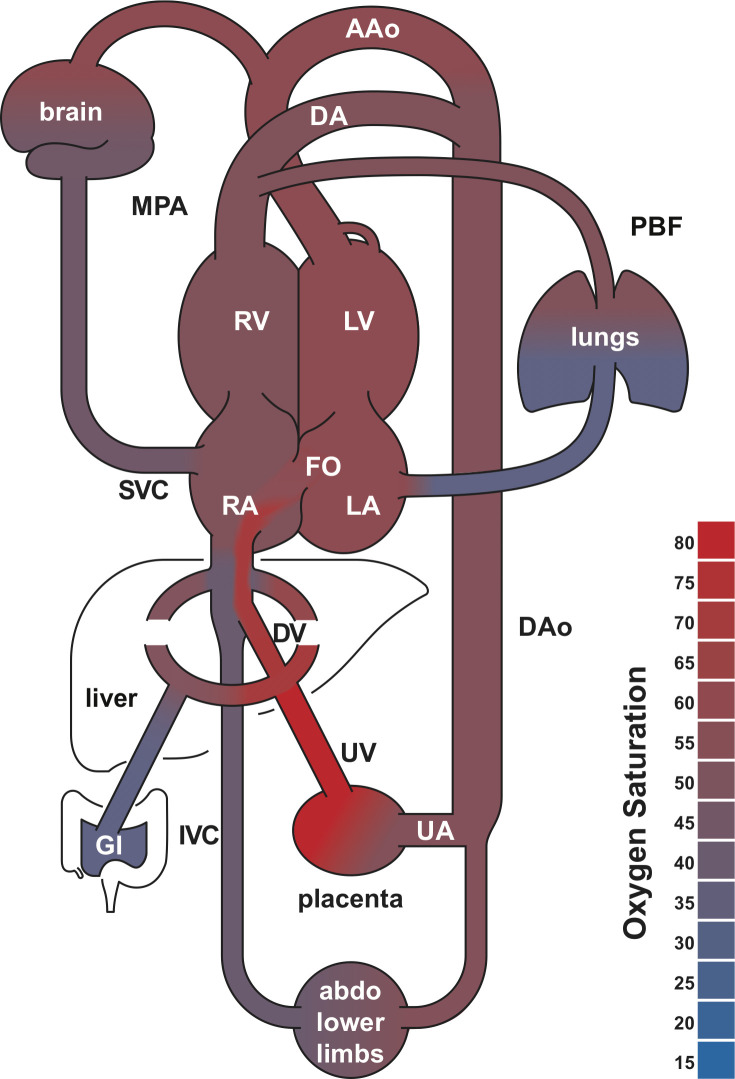
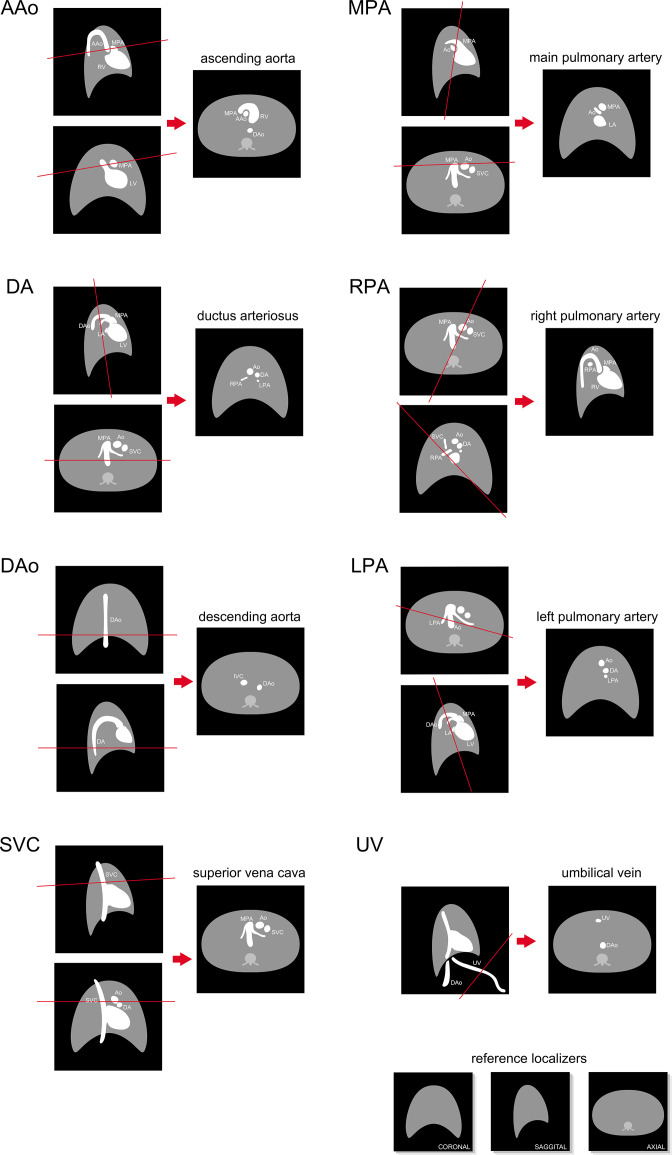
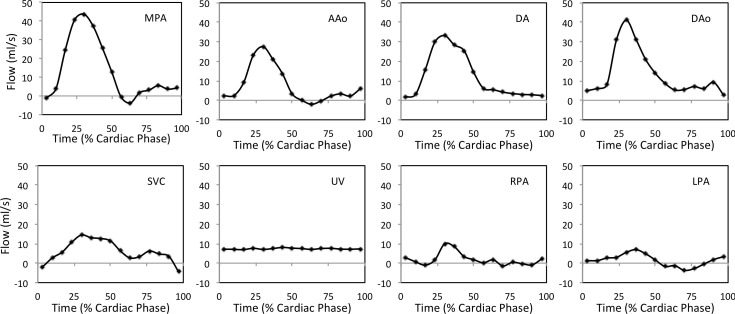
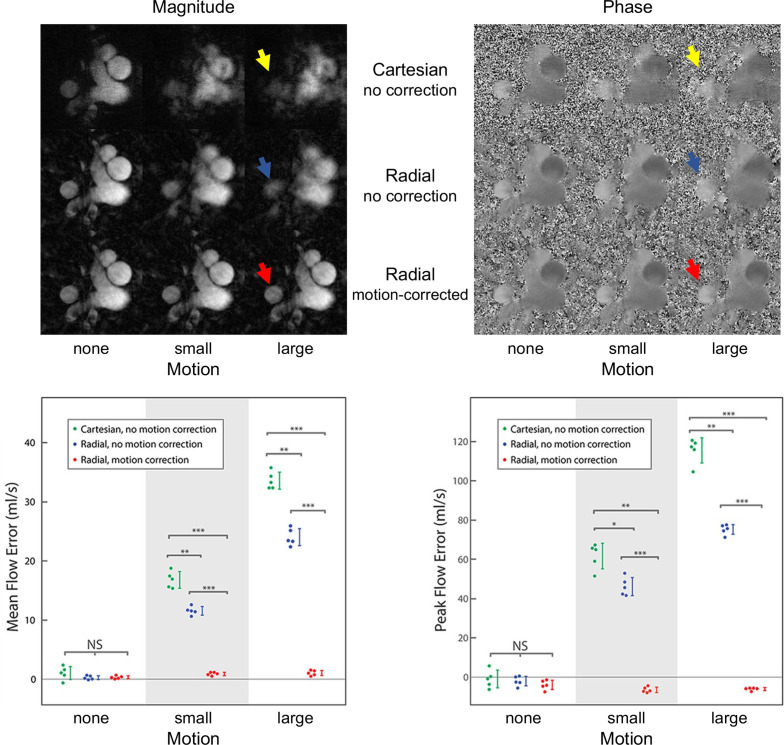
Fetal cardiac MRI is challenging due to fetal and maternal movements as well as the need for a reliable cardiac gating signal and high spatiotemporal resolution. Ongoing research and recent technical developments to address these challenges show the potential of MRI as an adjunct to ultrasound for the assessment of the fetal heart and great vessels. MRI measurements of blood flow have enabled the assessment of normal fetal circulation as well as conditions with disrupted circulations, such as congenital heart disease, along with associated organ underdevelopment and hemodynamic instability. This review provides details of the techniques used in fetal cardiovascular blood flow MRI, including single slice and volumetric imaging sequences, post-processing and analysis, along with a summary of applications in human studies and animal models.
Figures
References
-
- Yagel S, Silverman NH, Gembruch U, eds. Circulation in the normal fetus and cardiovascular adaptations to birth. Fetal Cardiology 2019; 119–37. Available from: 10.1201/9780429461118-16 - DOI
-
- Rudolph A. Fetal Cardiology. 3rd ed. CRC Press; 2019., pp.708–22. Available from: 10.1201/9780429461118-61 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
