

Impact of radiotherapy and sequencing of systemic therapy on survival outcomes in melanoma patients with previously untreated brain metastasis: a multicenter DeCOG study on 450 patients from the prospective skin cancer registry ADOREG
- PMID: 35688555
- PMCID: PMC9189852
- DOI: 10.1136/jitc-2022-004509
Impact of radiotherapy and sequencing of systemic therapy on survival outcomes in melanoma patients with previously untreated brain metastasis: a multicenter DeCOG study on 450 patients from the prospective skin cancer registry ADOREG
Abstract
Background: Despite of various therapeutic strategies, treatment of patients with melanoma brain metastasis (MBM) still is a major challenge. This study aimed at investigating the impact of type and sequence of immune checkpoint blockade (ICB) and targeted therapy (TT), radiotherapy, and surgery on the survival outcome of patients with MBM.
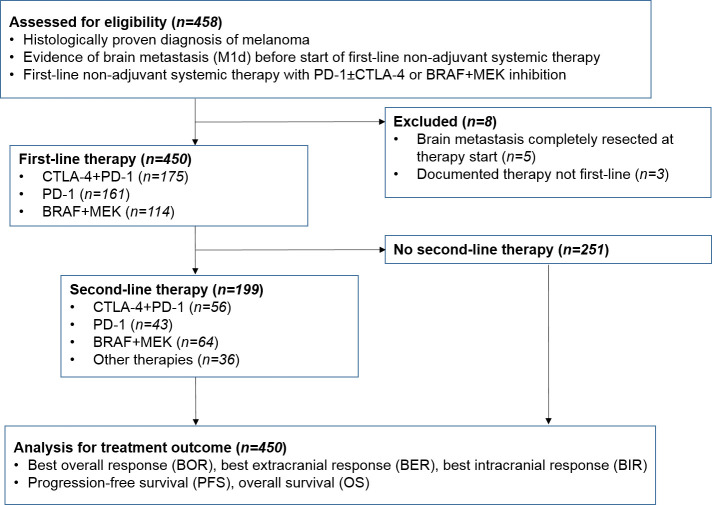
Method: We assessed data of 450 patients collected within the prospective multicenter real-world skin cancer registry ADOREG who were diagnosed with MBM before start of the first non-adjuvant systemic therapy. Study endpoints were progression-free survival (PFS) and overall survival (OS).
Results: Of 450 MBM patients, 175 (38.9%) received CTLA-4+PD-1 ICB, 161 (35.8%) PD-1 ICB, and 114 (25.3%) BRAF+MEK TT as first-line treatment. Additional to systemic therapy, 67.3% of the patients received radiotherapy (stereotactic radiosurgery (SRS); conventional radiotherapy (CRT)) and 24.4% had surgery of MBM. 199 patients (42.2%) received a second-line systemic therapy. Multivariate Cox regression analysis revealed the application of radiotherapy (HR for SRS: 0.213, 95% CI 0.094 to 0.485, p<0.001; HR for CRT: 0.424, 95% CI 0.210 to 0.855, p=0.016), maximal size of brain metastases (HR for MBM >1 cm: 1.977, 95% CI 1.117 to 3.500, p=0.019), age (HR for age >65 years: 1.802, 95% CI 1.016 to 3.197, p=0.044), and ECOG performance status (HR for ECOG ≥2: HR: 2.615, 95% CI 1.024 to 6.676, p=0.044) as independent prognostic factors of OS on first-line therapy. The type of first-line therapy (ICB vs TT) was not independently prognostic. As second-line therapy BRAF+MEK showed the best survival outcome compared with ICB and other therapies (HR for CTLA-4+PD-1 compared with BRAF+MEK: 13.964, 95% CI 3.6 to 54.4, p<0.001; for PD-1 vs BRAF+MEK: 4.587 95% CI 1.3 to 16.8, p=0.022 for OS). Regarding therapy sequencing, patients treated with ICB as first-line therapy and BRAF+MEK as second-line therapy showed an improved OS (HR for CTLA-4+PD-1 followed by BRAF+MEK: 0.370, 95% CI 0.157 to 0.934, p=0.035; HR for PD-1 followed by BRAF+MEK: 0.290, 95% CI 0.092 to 0.918, p=0.035) compared with patients starting with BRAF+MEK in first-line therapy. There was no significant survival difference when comparing first-line therapy with CTLA-4+PD-1 ICB with PD-1 ICB.
Conclusions: In patients with MBM, the addition of radiotherapy resulted in a favorable OS on systemic therapy. In BRAF-mutated MBM patients, ICB as first-line therapy and BRAF+MEK as second-line therapy were associated with a significantly prolonged OS.
Keywords: Immunotherapy; Melanoma; Radiotherapy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The authors declare no competing interests in reference to this work. For conflicts of interest outside the submitted work see list: CF has been on the advisory board or has received honoraria from Bristol Myers Squibb, Immunocore and Novartis and received travel grants from Bristol Myers Squibb, Novartis and Pierre Fabre. PM declares research support from Bristol Myers Squibb, Novartis and Merck Sharp & Dome; speakers and advisory board honoraria from Almirall Hermal, Beiersdorf, Bristol Myers Squibb, Merck Sharp & Dome, Immunocore, Merck Serono, Medac, Novartis, Pierre Fabre, Sanofi Genzyme, Sun Pharma and Roche, and travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis and Pierre Fabre. LB received honoraria from Amgen, Bristol Myers Squibb and Sun Pharma. IG declares speakers and advisory board honoraria from Almirall Hermal, Bristol Myers Squibb, Merck Sharp & Dome, Novartis, Pierre Fabre, Sanofi Genzyme, Sun Pharma and Roche. FM has received travel support or/and speaker’s fees or/and advisor’s honoraria by Novartis, Roche, BMS, MSD and Pierre Fabre and research funding from Novartis and Roche. RH reports speakers and advisory board honoraria from Bristol Myers Squibb (BMS), Immunocore, Novartis, Pierre-Fabre, Roche and SUN pharma. CP received honoraria (speaker honoraria or honoraria as a consultant) and travel support from: Novartis, BMS, Roche, Merck Serono, MSD, Celgene, AbbVie, SUNPHARMA, UCB, Allergy Therapeutics, Pierre Fabre, Kyowa Kirin and LEO. JUl has received research support from Novartis; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Roche, Pierre Fabre, and travel support from Bristol Myers Squibb and medac. PT declares speakers and advisory board honoraria from Almirall, Bristol Myers Squibb, Novartis, Merck Sharp & Dohme, Pierre-Fabre, CureVac, Merck Serono, Sanofi, Roche, Kyowa Kirin, Biofrontera and 4SC; travel support from Bristol Myers Squibb and Pierre-Fabre. DN has received advisory and speaker honoraria from Merck Sharp & Dome, Bristol Myers Squibb, Novartis, Almirall and Sanofi. AF Advisory Board: Roche, Novartis, MSD, BMS, Pierre-Fabre; support for congress participation: Roche, Novartis, BMS, Pierre-Fabre; speaker honoraria: Roche, Novartis, BMS, MSD, CeGaT; institutional research support BMS Stiftung Immunonkologie. JUt is on the advisory board or has received honoraria and travel support from Amgen, Bristol Myers Squibb, GSK, Immunocore, LeoPharma, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche and Sanofi. TG has received speakers and/or advisory board honoraria and travel support from BMS, Sanofi-Genzyme, MSD, Novartis Pharma, Roche, Abbvie, Almirall, Janssen, Lilly, Pfizer, Pierre Fabre, and Merck-Serono. FM served as consultant and/or has received honoraria from Novartis, Roche, Bristol Myers Squibb, Merck Sharp & Dohme, Pierre Fabre, Sanofi Genzyme and travel support from Novartis, Sunpharma and Bristol Myers Squibb. JW received honoraria from Pierre Fabre, Novartis and Merck Sharp & Dohme. KS has been on the advisory board or has received honoraria from Bristol Myers Squibb, Roche, Merck Sharp & Dome, Pierre Fabre, Novartis and received travel grants from Bristol Myers Squibb, Novartis and Pierre Fabre. IH has been on the advisory board of Ymmunobio. AR reported grants from Novartis, Bristol Myers Squibb, and Adtec; personal fees from Merck Sharp & Dohme; and non-financial support from Amgen, Roche, Merck Sharp & Dohme, Novartis, Bristol Myers Squibb, and Teva. LZ served as consultant and/or has received honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, Sunpharma and Sanofi; research funding to institution: Novartis; travel support from Merck Sharp & Dohme, Bristol Myers Squibb, Amgen, Pierre-Fabre, Sunpharma, Sanofi and Novartis. EL served as consultant and/or has received honoraria from Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Medac, Sanofi, Sunpharma and travel support from Medac, Bristol Myers Squibb, Pierre Fabre, Sunpharma and Novartis. DS: relevant financial activities (Roche, Novartis, Bristol Myers Squibb, Merck Sharp & Dohme, Sanofi, Regeneron, Array, Pierre Fabre, 4SC, Helsinn, Philogen, InFlarX, Merck-Serono, SunPharma, Ultimovacs, and Sandoz). SU declares research support from Bristol Myers Squibb and Merck Serona; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dome, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, Merck Sharp & Dohme and Pierre Fabre. All other authors have no conflict of interest to declare.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials