

Peripheral blood immune cell dynamics reflect antitumor immune responses and predict clinical response to immunotherapy
- PMID: 35688557
- PMCID: PMC9189831
- DOI: 10.1136/jitc-2022-004688
Peripheral blood immune cell dynamics reflect antitumor immune responses and predict clinical response to immunotherapy
Abstract
Background: Despite treatment advancements with immunotherapy, our understanding of response relies on tissue-based, static tumor features such as tumor mutation burden (TMB) and programmed death-ligand 1 (PD-L1) expression. These approaches are limited in capturing the plasticity of tumor-immune system interactions under selective pressure of immune checkpoint blockade and predicting therapeutic response and long-term outcomes. Here, we investigate the relationship between serial assessment of peripheral blood cell counts and tumor burden dynamics in the context of an evolving tumor ecosystem during immune checkpoint blockade.
Methods: Using machine learning, we integrated dynamics in peripheral blood immune cell subsets, including neutrophil-lymphocyte ratio (NLR), from 239 patients with metastatic non-small cell lung cancer (NSCLC) and predicted clinical outcome with immune checkpoint blockade. We then sought to interpret NLR dynamics in the context of transcriptomic and T cell repertoire trajectories for 26 patients with early stage NSCLC who received neoadjuvant immune checkpoint blockade. We further determined the relationship between NLR dynamics, pathologic response and circulating tumor DNA (ctDNA) clearance.
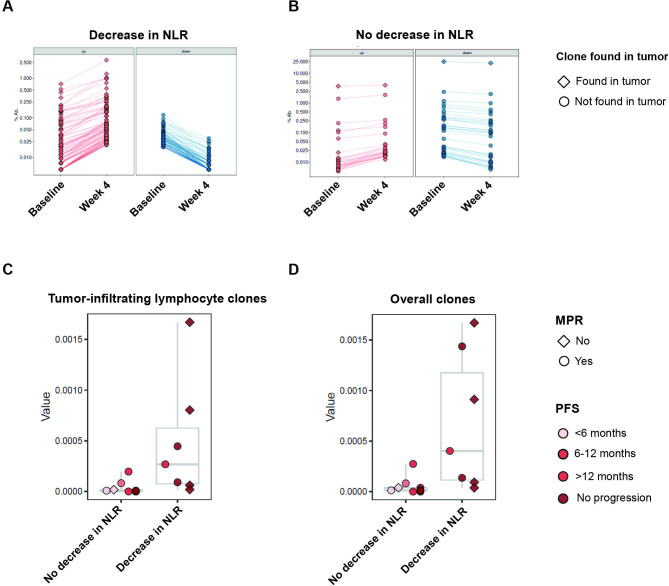
Results: Integrated dynamics of peripheral blood cell counts, predominantly NLR dynamics and changes in eosinophil levels, predicted clinical outcome, outperforming both TMB and PD-L1 expression. As early changes in NLR were a key predictor of response, we linked NLR dynamics with serial RNA sequencing deconvolution and T cell receptor sequencing to investigate differential tumor microenvironment reshaping during therapy for patients with reduction in peripheral NLR. Reductions in NLR were associated with induction of interferon-γ responses driving the expression of antigen presentation and proinflammatory gene sets coupled with reshaping of the intratumoral T cell repertoire. In addition, NLR dynamics reflected tumor regression assessed by pathological responses and complemented ctDNA kinetics in predicting long-term outcome. Elevated peripheral eosinophil levels during immune checkpoint blockade were correlated with therapeutic response in both metastatic and early stage cohorts.
Conclusions: Our findings suggest that early dynamics in peripheral blood immune cell subsets reflect changes in the tumor microenvironment and capture antitumor immune responses, ultimately reflecting clinical outcomes with immune checkpoint blockade.
Keywords: immunotherapy; translational medical research; tumor biomarkers.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: VA receives research funding to her institution from Bristol-Myers Squibb and Astra Zeneca. PMF has received research funding to his institution from AstraZeneca, Bristol-Myers Squibb, Novartis, Corvus, Kyowa. He has also served as a consultant for Amgen, AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Iteos, Janssen, Mirati, Novartis, Sanofi and as a DSMB member for Polaris and Flame Therapeutics. KNS receives research funding to her institution from Bristol-Myers Squibb, Astra Zeneca, and Enara Bio, and holds founder’s equity in manaT Bio. VEV is a founder of Delfi Diagnostics and Personal Genome Diagnostics, serves on the Board of Directors and as a consultant for both organizations, and owns Delfi Diagnostics and Personal Genome Diagnostics stock, which are subject to certain restrictions under university policy. Additionally, Johns Hopkins University owns equity in Delfi Diagnostics and Personal Genome Diagnostics. VEV is an inventor of multiple licensed patents related to technologies from Johns Hopkins University. Some of these licenses and relationships are associated with equity or royalty payments directly to Johns Hopkins and VEV. VEV is an advisor to Bristol-Myers Squibb, Danaher, Genentech, and Takeda Pharmaceuticals. Within the last five years, VEV has been an advisor to Merck and Ignyta. These arrangements have been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. JW is a consultant for Personal Genome Diagnostics, is the founder and owner of Resphera Biosciences and holds patents, royalties or other intellectual property from Personal Genomic Diagnostics. JER is in the advisory board/consultant of Oncocyte, receives speaking fees for Astrazeneca, and has received research funding to his institution from Genetech/Roche, and Verastem. JB is in the advisory board/consultant of Amgen, AstraZeneca, BMS, Genentech/Roche, Eli Lilly, GlaxoSmithKline, Merck, Sanofi and Regeneron, receives grant research funding from AstraZeneca, BMS, Genentech/Roche, Merck, RAPT Therapeutics, Inc and Revolution Medicines and is in the Data and Safety Monitoring Board/Committees of GlaxoSmithKline, Sanofi and Janssen. TS is in the advisory board/consultant of Cue Biopharma, Dracen, Innate, Nanobiotix, Merck, Sanofi, Synthekine, receives grant research funding from AstraZeneca, BMS, Cue Biopharma, Genentech/Roche, Merck, Nanobiotix, Synthekine, and is in the Data and Safety Monitoring Board/Committees of Astra Zeneca, and Nektar. VL has received research funding to his institution from AstraZeneca, Bristol-Myers Squibb, Merck, SeaGen. He has also served as a consultant for Takeda, SeaGen, Bristol-Myers Squibb, AstraZeneca, and Guardant Health.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials