

Medicaid Expansion and Contraceptive Use Among Female High-School Students
- PMID: 35688721
- PMCID: PMC10926112
- DOI: 10.1016/j.amepre.2022.04.020
Medicaid Expansion and Contraceptive Use Among Female High-School Students
Abstract
Introduction: Access to effective contraception prevents unintended pregnancies among sexually active female youth. Potentially impacted by the Affordable Care Act's Medicaid-related policies, contraception use increased among sexually active high-school students from 2013 to 2019.
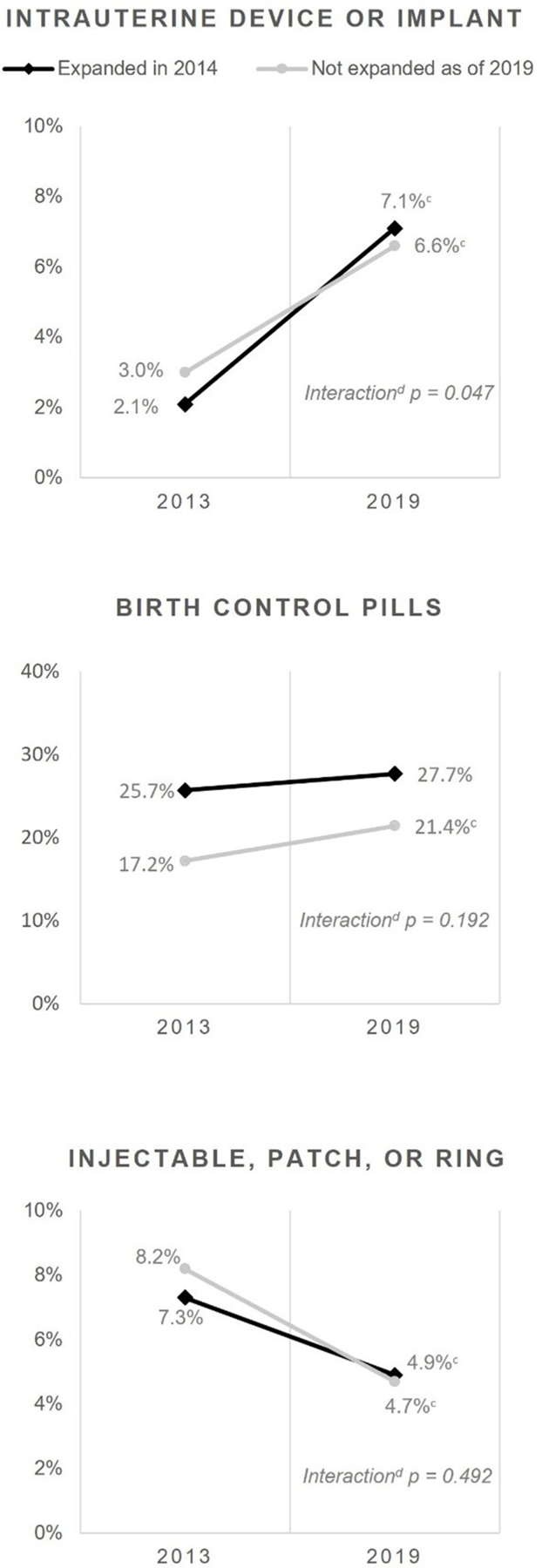
Methods: Analyses conducted in 2021 assessed state-level Youth Risk Behavior Survey data among female students in grades 9-12 who reported being sexually active. States that expanded Medicaid were compared with other states in 2013 (baseline) and 2019 (after expansion). Measured outcomes included self-reported use of moderately effective or highly effective, long-acting reversible contraception at last sex. Long-acting reversible contraception included intrauterine devices and implants. Moderately effective contraception included birth control pills, injectables, patches, or rings. Results were weighted and adjusted for age and race/ethnicity.
Results: Students in Medicaid expansion states (n=27,564) did not differ significantly from those in nonexpansion states (n=6,048) at baseline or after expansion with respect to age, age at first sex, or the number of sexual partners in the past 3 months; however, race/ethnicity population characteristics changed over time. Postexpansion increased use of intrauterine devices/implants was greater in Medicaid expansion states than in nonexpansion states (238.1% increase vs 120.0% increase, adjusted p=0.047). For those aged 16-17 years, Medicaid expansion states had a 283.3% increase in intrauterine device/implant use compared with an increase of 69.7% in nonexpansion states (adjusted p=0.004).
Conclusions: Medicaid expansion was associated with a greater population-level increase in intrauterine device/implant use among sexually active female high-school students aged 16-17 years. These findings point to the possibility that the Affordable Care Act's Medicaid-related policies played a role in young women's use of intrauterine devices/implants.
Published by Elsevier Inc.
Figures
References
-
- Trussell J, Aiken AR, Micks E, Guthrie KA. Efficacy, safety, and personal considerations. Contraceptive Technology Mishawaka, IN: Ayer Company Publishers, Inc., 2018.
-
- Centers for Disease Control and Prevention. Youth Risk Behavior Survey Data Summary & Trends Report 2009–2019 Atlanta, GA: Centers for Disease Control and Prevention, 2019. https://www.cdc.gov/healthyyouth/data/yrbs/pdf/YRBSDataSummaryTrendsRepo.... Accessed May 5, 2022.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
