

Mouthwash as a non-invasive method of indocyanine green delivery for near-infrared fluorescence dental imaging
- PMID: 35689334
- PMCID: PMC9186466
- DOI: 10.1117/1.JBO.27.6.066001
Mouthwash as a non-invasive method of indocyanine green delivery for near-infrared fluorescence dental imaging
Abstract
Significance: X-ray imaging serves as the mainstream imaging in dentistry, but it involves risk of ionizing radiation.
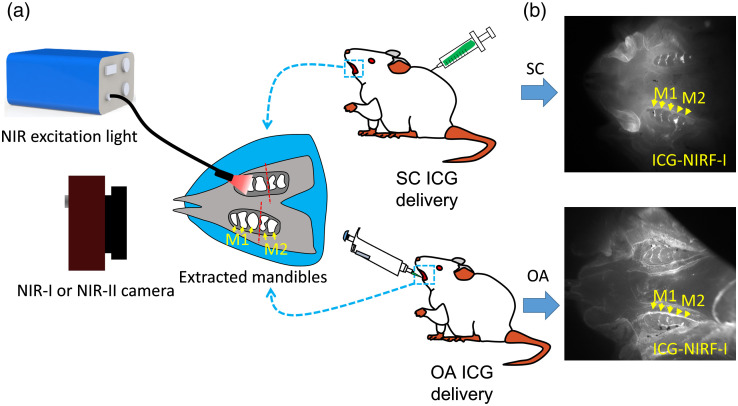
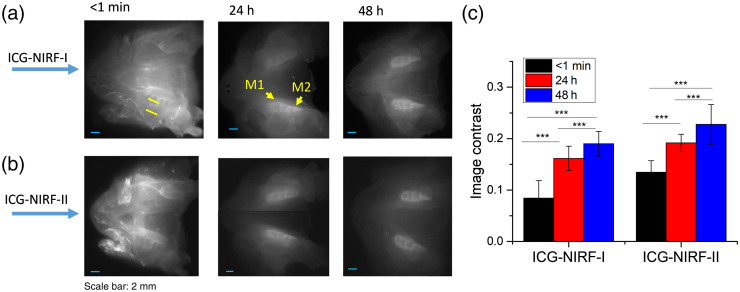
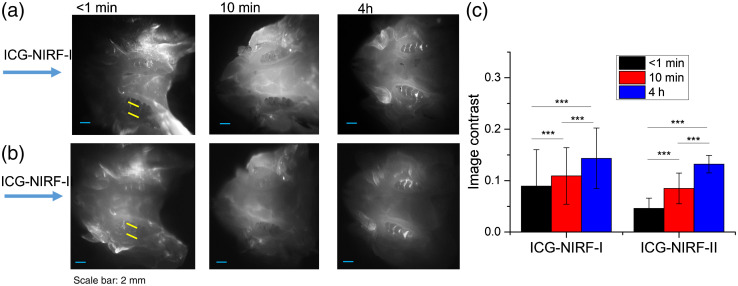
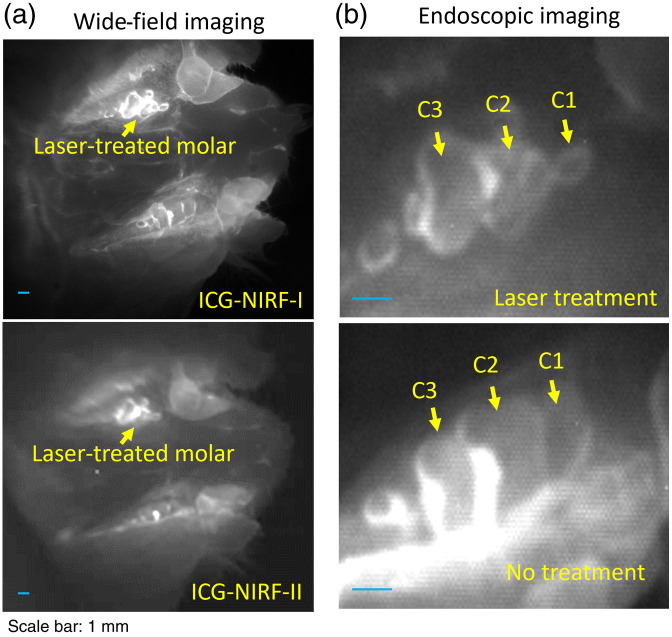
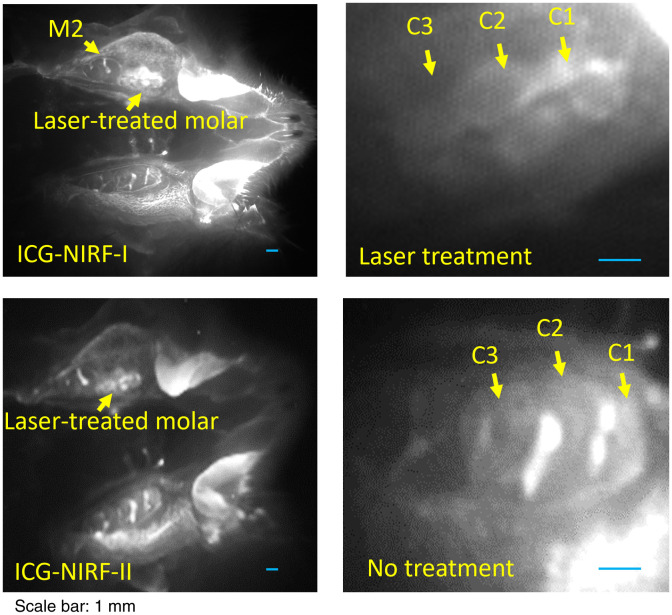
Aim: This study presents the feasibility of indocyanine green-assisted near-infrared fluorescence (ICG-NIRF) dental imaging with 785-nm NIR laser in the first (ICG-NIRF-I: 700 to 1000 nm) and second (ICG-NIRF-II: 1000 to 1700 nm) NIR wavelengths.
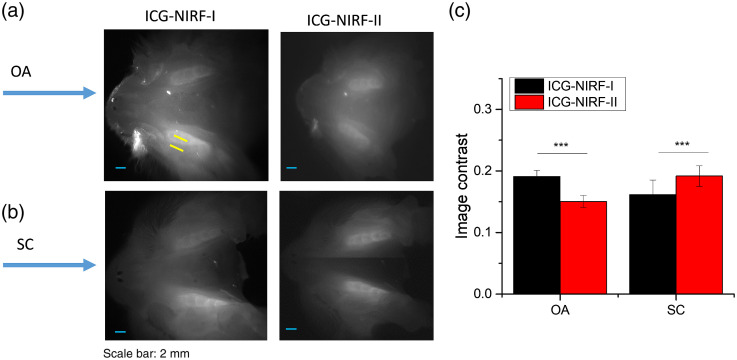
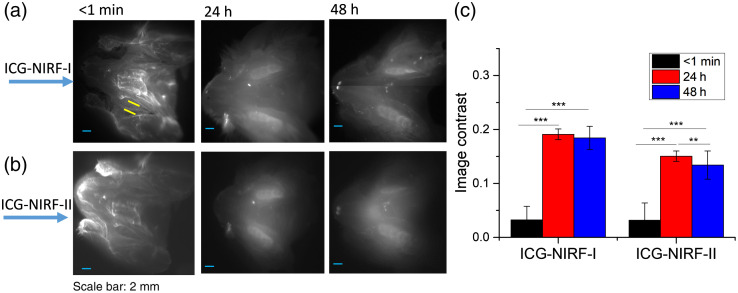
Approach: Sprague Dawley rats with different postnatal days were used as animal models. ICG, as a fluorescence agent, was delivered to dental structures by subcutaneous injection (SC) and oral administration (OA).
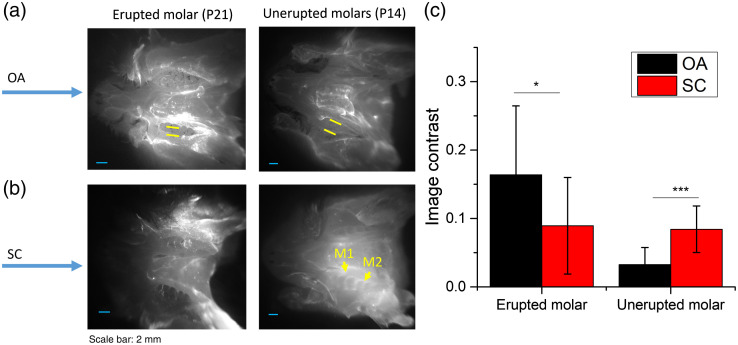
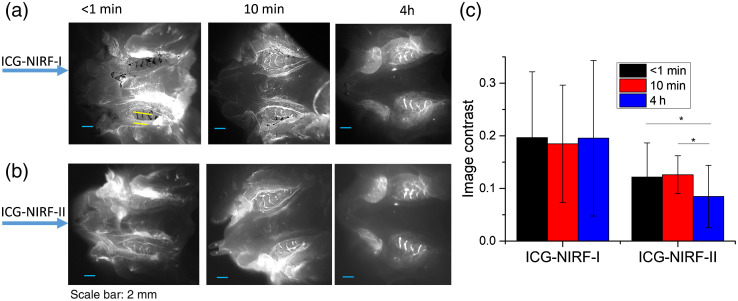
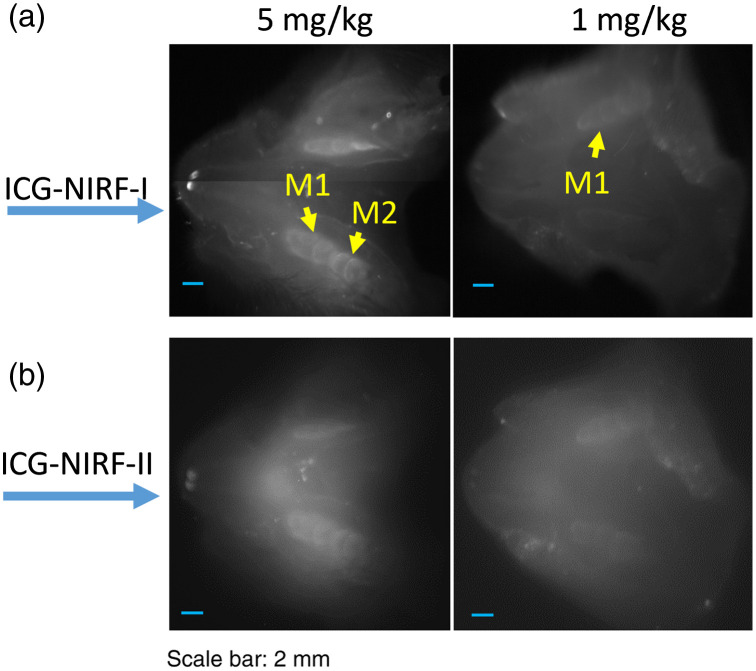
Results: For SC method, erupted and unerupted molars could be observed from ICG-NIRF images at a short imaging time (<1 min). ICG-NIRF-II could achieve a better image contrast in unerupted molars at 24 h after ICG injection. The OA could serve as a non-invasive method for ICG delivery; it could also cause the glow-in-dark effect in unerupted molars. For erupted molars, OA can be considered as mouthwash and exhibits outstanding performance for delivery of ICG dye; erupted molar structures could be observed at a short imaging time (<1 min) and low ICG dose (0.05 mg / kg).
Conclusions: Overall, ICG-NIRF with mouthwash could perform in-vivo dental imaging in two NIR wavelengths at a short time and low ICG dose.
Keywords: indocyanine green; indocyanine green delivery; mouthwash; near-infrared fluorescence dental imaging; oral administration.
Figures

References
-
- A. D. Association, Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure, ADA, Chicago: (2012).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
