

A BURST-BAUS consensus document for best practice in the conduct of scrotal exploration for suspected testicular torsion: the Finding consensus for orchIdopeXy In Torsion (FIX-IT) study
- PMID: 35689399
- PMCID: PMC9796508
- DOI: 10.1111/bju.15818
A BURST-BAUS consensus document for best practice in the conduct of scrotal exploration for suspected testicular torsion: the Finding consensus for orchIdopeXy In Torsion (FIX-IT) study
Abstract
Objectives: To produce a best practice consensus guideline for the conduct of scrotal exploration for suspected testicular torsion using formal consensus methodology.
Materials and methods: A panel of 16 expert urologists, representing adult, paediatric, general, and andrological urology used the RAND/UCLA Appropriateness Consensus Methodology to score a 184 statement pre-meeting questionnaire on the conduct of scrotal exploration for suspected testicular torsion. The collated responses were presented at a face-to-face online meeting and each item was rescored anonymously after a group discussion, facilitated by an independent chair with expertise in consensus methodology. Items were scored for agreement and consensus and the items scored with consensus were used to derive a set of best practice guidelines.
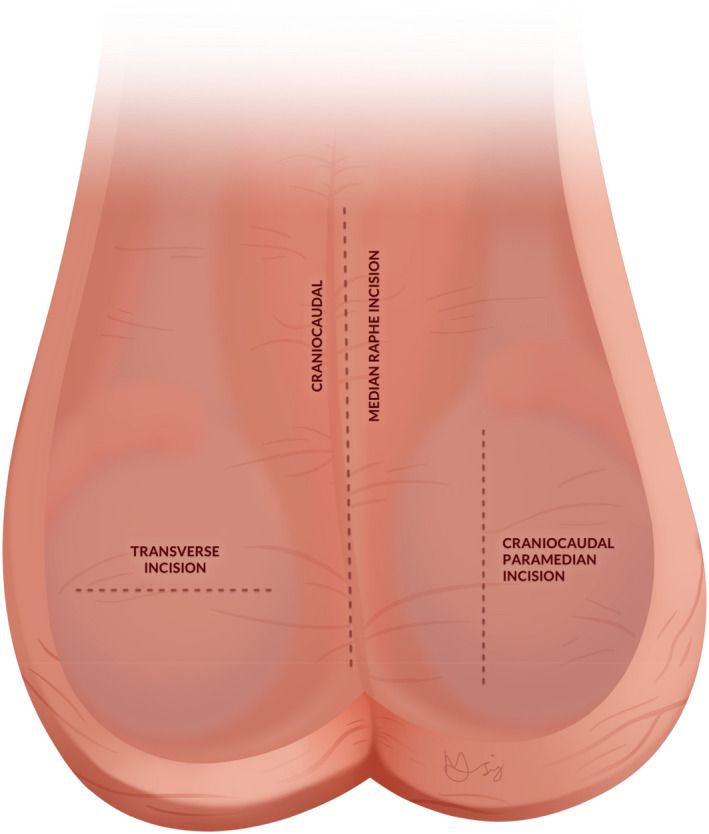
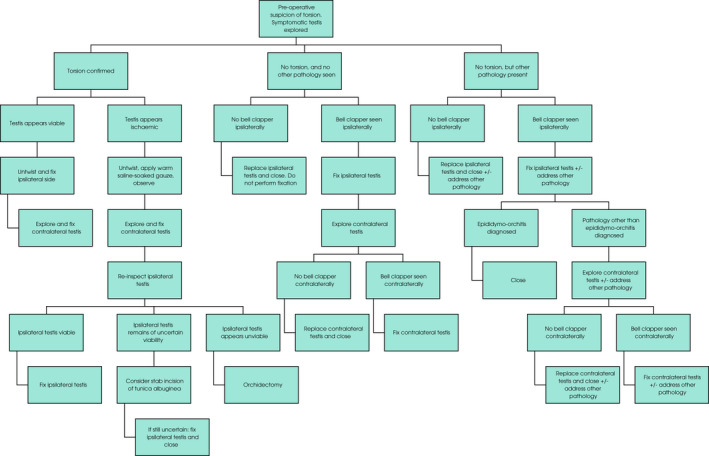
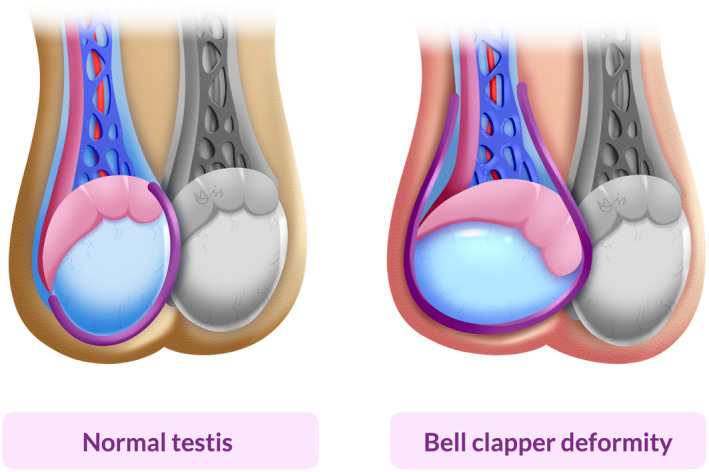
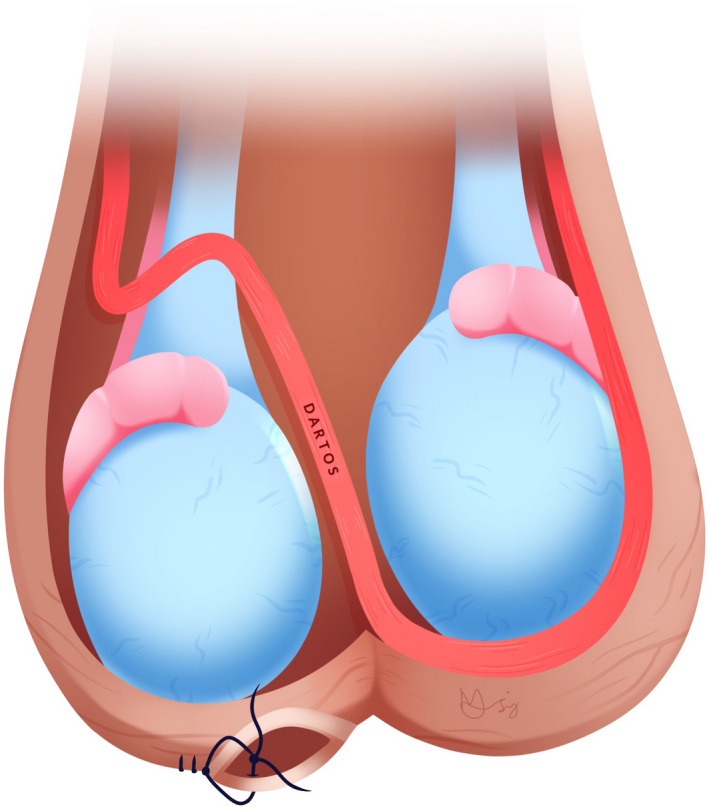
Results: Statements scored as with consensus increased from Round 1 (122/184, 66.3%) to Round 2 (149/200, 74.5%). Recommendations were generated in ten categories: consent, assessment under anaesthetic, initial incision, intraoperative decision making, fixation, medical photography, closure, operation note, logistics and follow-up after scrotal exploration. Our statements assume that the decision to operate has already been made. Key recommendations in the consent process included the discussion of the possibility of orchidectomy and the possibility of subsequent infection of the affected testis or wound requiring antibiotic therapy. If after the examination under anaesthesia, the index of suspicion of testicular torsion is lower than previously thought, then the surgeon should still proceed to scrotal exploration as planned. A flow chart guiding decision making dependent on intraoperative findings has been designed. If no torsion is present on exploration and the bell clapper deformity is absent, the testis should not be fixed. When fixing a testis using sutures, 3 or 4-point is acceptable and non-absorbable sutures are preferred.
Conclusions: We have produced consensus recommendations to inform best practice in the conduct of scrotal exploration for suspected testicular torsion.
Keywords: Fixation; Orchidopexy; Scrotal exploration; Surgical Technique; Testicular Torsion.
This article is protected by copyright. All rights reserved.
Figures
Comment in
-
Re: a BURST-BAUS consensus document: FIX-IT study.BJU Int. 2023 Apr;131(4):513. doi: 10.1111/bju.15977. Epub 2023 Feb 3. BJU Int. 2023. PMID: 36734096 No abstract available.
References
-
- Mellick LB, Sinex JE, Gibson RW, Mears K. A systematic review of testicle survival time after a torsion event. Pediatr Emerg Care 2019; 35: 821–5 - PubMed
-
- Moore SL, Chebbout R, Cumberbatch M et al. Orchidopexy for testicular torsion: A systematic review of surgical technique. Eur Urol Focus 2020; 7: 1493–503 - PubMed
-
- European Association of Urology . Paediatric urology. 2020. Available at: https://uroweb.org/guideline/paediatric‐urology/. Accessed 21 March 2021
