

Strategic infarct location for post-stroke seizure
- PMID: 35689977
- PMCID: PMC9190039
- DOI: 10.1016/j.nicl.2022.103069
Strategic infarct location for post-stroke seizure
Abstract
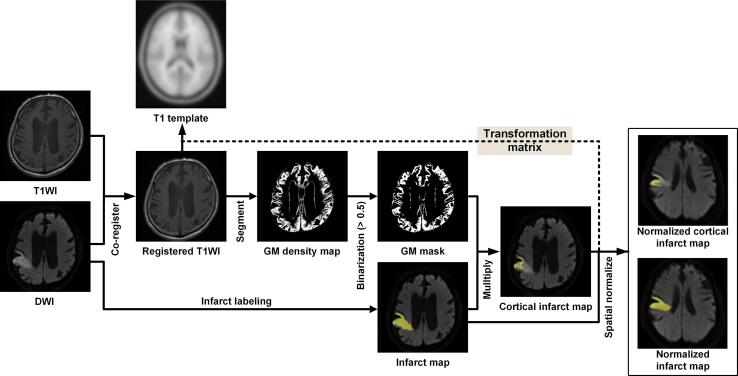
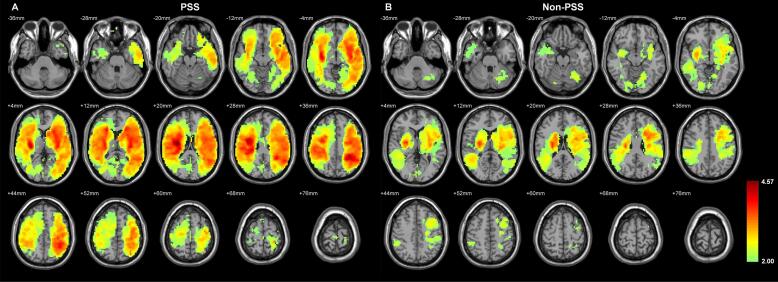
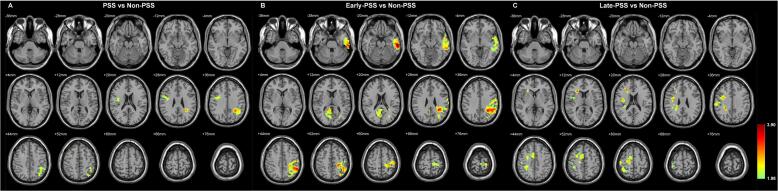
Post-stroke seizure (PSS) can have a strong negative impact on functional recovery after stroke. Researchers have identified numerous risk factors of PSS; however, the relationship between infarction location and PSS remains unclear. We recruited patients who presented with an acute cerebral infarction between 2012 and 2017 and suffered from seizures within 1 year after stroke (PSS group). PSS group was subgrouped into early-PSS and late-PSS groups based on the interval between seizure and stroke. We also recruited an equal number of acute cerebral infarction patients without post-stroke seizures during the follow-up period (Non-PSS group). All brain MRIs from the two groups were processed, whereupon normalized infarct maps from the PSS and Non-PSS groups were compared via voxel- and volumetric-based analyses. A total of 132 subjects were enrolled in the study, including PSS (n = 66, consisting of 31 early-PSS and 35 late-PSS) and Non-PSS (n = 66) patients. No significant differences were observed between the two groups in terms of stroke lateralization or severity. Image analysis revealed that the volume of infarction was larger in the PSS group than in the Non-PSS group; however, the difference did not reach the level of significance. Unlike the Non-PSS group, the PSS group presented hot spots over the left central region, left superior parietal lobule, and right frontal operculum. We observed differences between the distribution of hot spots among patients with early-PSS and those with late-PSS. We found that some brain regions were significantly associated with the development of PSS after ischemic stroke, and these regions differed between cases of early and late PSS. It appears that the location of infarction could help clinicians assess the risk of PSS in specific post-stroke stages.
Keywords: Cerebral infarction; Epileptogenesis; Ischemic stroke; Post-stroke epilepsy; Risk factors.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Ashburner J., Friston K.J. Unified segmentation. Neuroimage. 2005;26:839–851. - PubMed
-
- Bladin C.F., Alexandrov A.V., Bellavance A., Bornstein N., Chambers B., Coté R., Lebrun L., Pirisi A., Norris J.W. Seizures after stroke: A prospective multicenter study. Arch. Neurol. 2000;57:1617–1622. - PubMed
-
- de Palma L., De Benedictis A., Specchio N., Marras C.E. Epileptogenic network formation. Neurosurg. Clin. N. Am. 2020;31:335–344. - PubMed
-
- Ferreira-Atuesta C., Döhler N., Erdélyi-Canavese B., Felbecker A., Siebel P., Scherrer N., Bicciato G., Schweizer J., Sinka L., Imbach L.L., Katan M., Abraira L., Santamarina E., Álvarez-Sabín J., Winklehner M., von Oertzen T.J., Wagner J.N., Gigli G.L., Serafini A., Janes F., Merlino G., Valente M., Gregoraci G., Conrad J., Evers S., Lochner P., Roell F., Brigo F., Bentes C., Peralta A.R., Melo T.P.E., Keezer M.R., Duncan J.S., Sander J.W., Tettenborn B., Koepp M.J., Galovic M. Seizures after ischemic stroke: A matched multicenter study. Ann. Neurol. 2021;90:808–820. - PMC - PubMed
Further reading
-
- Kammersgaard L.P., Olsen T.S. Poststroke epilepsy in the copenhagen stroke study: Incidence and predictors. J. Stroke Cerebrovasc Dis. 2005;14:210–214. - PubMed
-
- Lossius M.I., Rønning O.M., Mowinckel P., Gjerstad L. Incidence and predictors for post-stroke epilepsy. A prospective controlled trial. the akershus stroke study. Eur. J. Neurol. 2002;9:365–368. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
