

Effect of priming interval on reactogenicity, peak immunological response, and waning after homologous and heterologous COVID-19 vaccine schedules: exploratory analyses of Com-COV, a randomised control trial
- PMID: 35690076
- PMCID: PMC9179150
- DOI: 10.1016/S2213-2600(22)00163-1
Effect of priming interval on reactogenicity, peak immunological response, and waning after homologous and heterologous COVID-19 vaccine schedules: exploratory analyses of Com-COV, a randomised control trial
Abstract
Background: Priming COVID-19 vaccine schedules have been deployed at variable intervals globally, which might influence immune persistence and the relative importance of third-dose booster programmes. Here, we report exploratory analyses from the Com-COV trial, assessing the effect of 4-week versus 12-week priming intervals on reactogenicity and the persistence of immune response up to 6 months after homologous and heterologous priming schedules using the vaccines BNT162b2 (tozinameran, Pfizer/BioNTech) and ChAdOx1 nCoV-19 (AstraZeneca).
Methods: Com-COV was a participant-masked, randomised immunogenicity trial. For these exploratory analyses, we used the trial's general cohort, in which adults aged 50 years or older were randomly assigned to four homologous and four heterologous vaccine schedules using BNT162b2 and ChAdOx1 nCoV-19 with 4-week or 12-week priming intervals (eight groups in total). Immunogenicity analyses were done on the intention-to-treat (ITT) population, comprising participants with no evidence of SARS-CoV-2 infection at baseline or for the trial duration, to assess the effect of priming interval on humoral and cellular immune response 28 days and 6 months post-second dose, in addition to the effects on reactogenicity and safety. The Com-COV trial is registered with the ISRCTN registry, 69254139 (EudraCT 2020-005085-33).
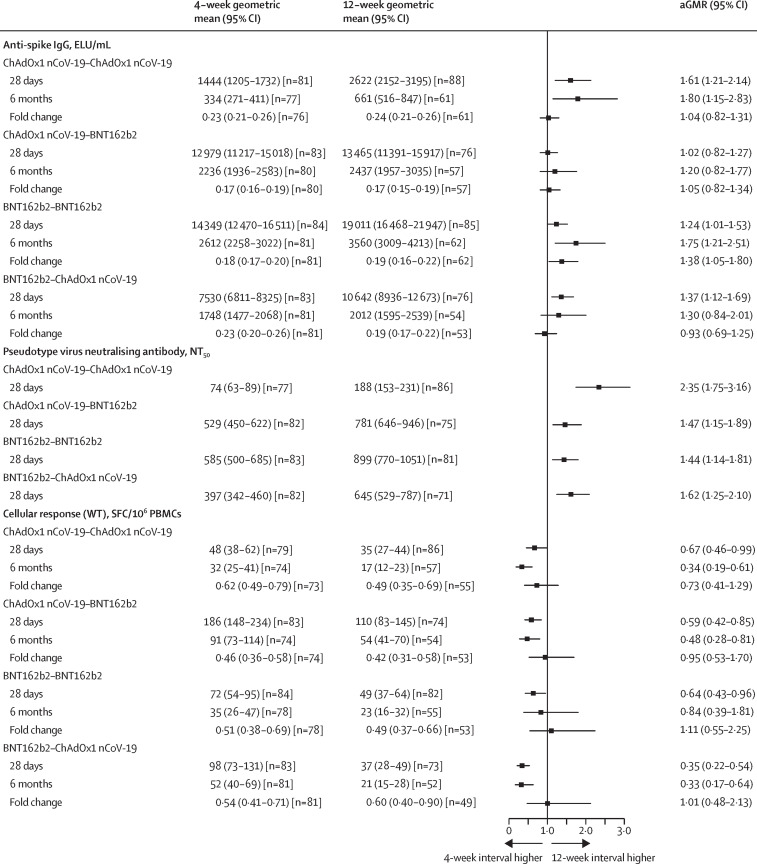
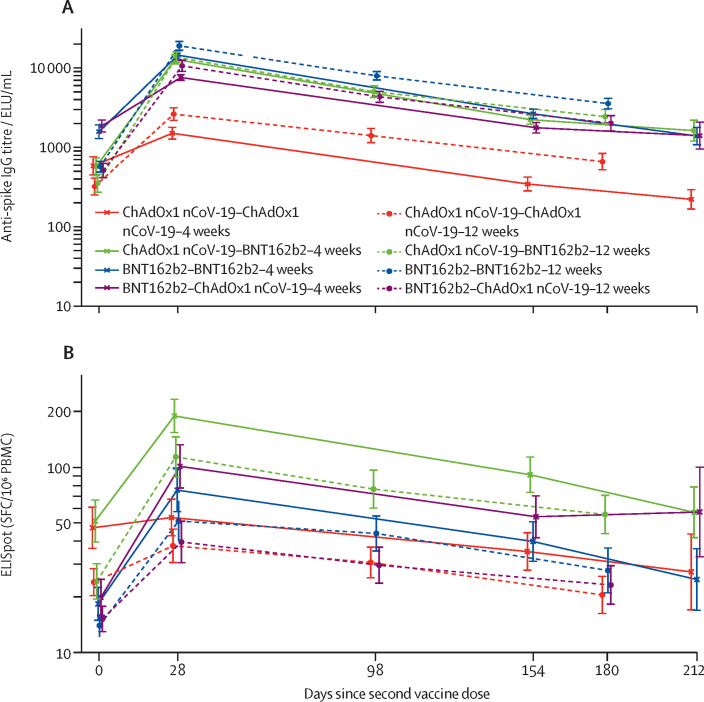
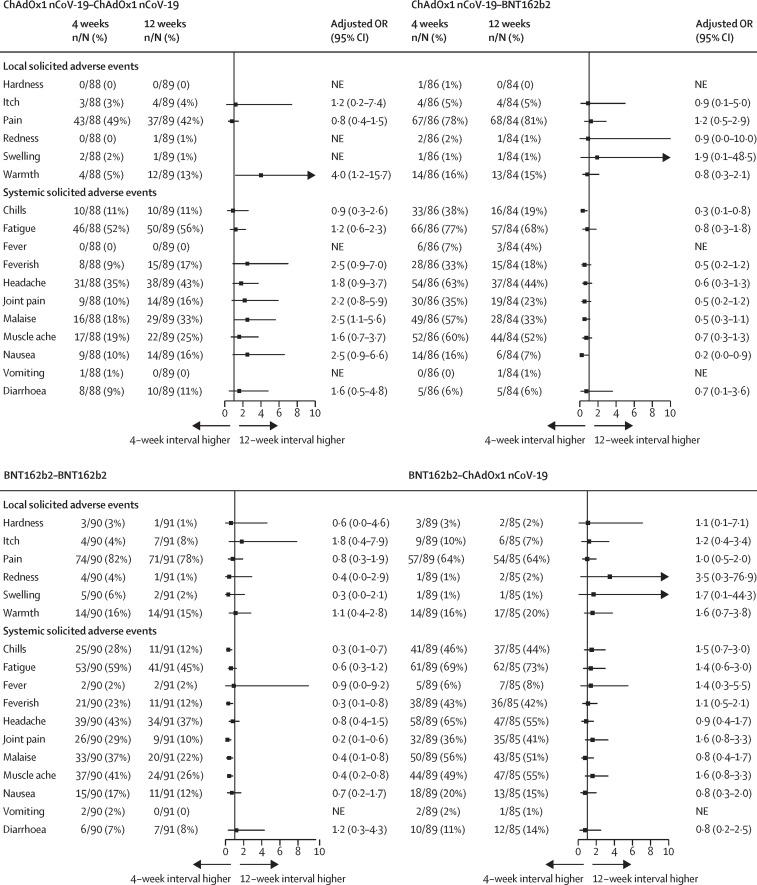
Findings: Between Feb 11 and 26, 2021, 730 participants were randomly assigned in the general cohort, with 77-89 per group in the ITT analysis. At 28 days and 6 months post-second dose, the geometric mean concentration of anti-SARS-CoV-2 spike IgG was significantly higher in the 12-week interval groups than in the 4-week groups for homologous schedules. In heterologous schedule groups, we observed a significant difference between intervals only for the BNT162b2-ChAdOx1 nCoV-19 group at 28 days. Pseudotyped virus neutralisation titres were significantly higher in all 12-week interval groups versus 4-week groups, 28 days post-second dose, with geometric mean ratios of 1·4 (95% CI 1·1-1·8) for homologous BNT162b2, 1·5 (1·2-1·9) for ChAdOx1 nCoV-19-BNT162b2, 1·6 (1·3-2·1) for BNT162b2-ChAdOx1 nCoV-19, and 2·4 (1·7-3·2) for homologous ChAdOx1 nCoV-19. At 6 months post-second dose, anti-spike IgG geometric mean concentrations fell to 0·17-0·24 of the 28-day post-second dose value across all eight study groups, with only homologous BNT162b2 showing a slightly slower decay for the 12-week versus 4-week interval in the adjusted analysis. The rank order of schedules by humoral response was unaffected by interval, with homologous BNT162b2 remaining the most immunogenic by antibody response. T-cell responses were reduced in all 12-week priming intervals compared with their 4-week counterparts. 12-week schedules for homologous BNT162b2 and ChAdOx1 nCoV-19-BNT162b2 were up to 80% less reactogenic than 4-week schedules.
Interpretation: These data support flexibility in priming interval in all studied COVID-19 vaccine schedules. Longer priming intervals might result in lower reactogenicity in schedules with BNT162b2 as a second dose and higher humoral immunogenicity in homologous schedules, but overall lower T-cell responses across all schedules. Future vaccines using these novel platforms might benefit from schedules with long intervals.
Funding: UK Vaccine Taskforce and National Institute for Health and Care Research.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MDS acts on behalf of the University of Oxford as an investigator on studies funded or sponsored by vaccine manufacturers AstraZeneca, GlaxoSmithKline, Pfizer, Novavax, Janssen, Medimmune, and MCM vaccines, receiving no personal financial payment for this work. JSN-V-T was seconded to the Department of Health and Social Care (DHSC), England. AMC and DMF are investigators on studies funded by Pfizer and Unilever, receiving no personal financial payment for this work. AF is a member of the Joint Committee on Vaccination and Immunisation and Chair of the WHO European Technical Advisory Group of Experts on immunisation; he is an investigator, provides consultative advice, or both on clinical trials and studies of COVID-19 vaccines produced by AstraZeneca, Janssen, Valneva, Pfizer, and Sanofi and of other vaccines from these and other manufacturers GlaxoSmithKline, VPI, Takeda, and Bionet Asia, receiving no personal remuneration or benefits for any of this work. SNF acts on behalf of University Hospital Southampton NHS Foundation Trust as an investigator, provider of consultative advice, or both on clinical trials and studies of COVID-19 and other vaccines funded or sponsored by vaccine manufacturers Janssen, Pfizer, AstraZeneca, GlaxoSmithKline, Novavax, Seqirus, Sanofi, Medimmune, Merck, and Valneva vaccines and antimicrobials, receiving no personal financial payment for this work. PTH acts on behalf of St George's University of London as an investigator on clinical trials of COVID-19 vaccines funded or sponsored by vaccine manufacturers Janssen, Pfizer, AstraZeneca, Novavax, and Valneva, receiving no personal financial payment for this work. CAG acts on behalf of University Hospitals Birmingham NHS Foundation Trust as an investigator on clinical trials and studies of COVID-19 and other vaccines funded or sponsored by vaccine manufacturers Janssen, Pfizer, AstraZeneca, Novavax, CureVac, Moderna, and Valneva vaccines, receiving no personal financial payment for this work. VL acts on behalf of University College London Hospitals NHS Foundation Trust as an investigator on clinical trials of COVID-19 vaccines funded or sponsored by vaccine manufacturers Pfizer, AstraZeneca, and Valneva, receiving no personal financial payment for this work. TL is named as an inventor on a patent application covering this SARS-CoV-2 vaccine (GB2003670.3) and is an occasional consultant to Vaccitech, unrelated to this work. Oxford University has entered into a partnership with AstraZeneca for further development of ChAdOx1 nCoV-19.
Figures
References
-
- WHO Interim recommendations for heterologous COVID-19 vaccine schedules. 2021. https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE-reco...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
