

Zone 1 REBOA in a combat DCBI swine model does not worsen brain injury
- PMID: 35690490
- PMCID: PMC9675949
- DOI: 10.1016/j.surg.2022.04.055
Zone 1 REBOA in a combat DCBI swine model does not worsen brain injury
Abstract
Background: Zone 1 resuscitative endovascular balloon occlusion of the aorta has been recommended for refractory shock after a dismounted complex blast injury for the austere combat scenario. While resuscitative endovascular balloon occlusion of the aorta should enhance coronary perfusion, there is a potential risk of secondary brain injury due to loss of cerebral autoregulation. We developed a combat casualty relevant dismounted complex blast injury swine model to evaluate the effects of resuscitative endovascular balloon occlusion of the aorta zone I on intracranial pressure and cerebral edema. We hypothesized that zone 1 aortic occlusion with resuscitative endovascular balloon occlusion of the aorta would increase mean arterial pressure transmitted in excessive intracranial pressure, thereby worsening brain injury.
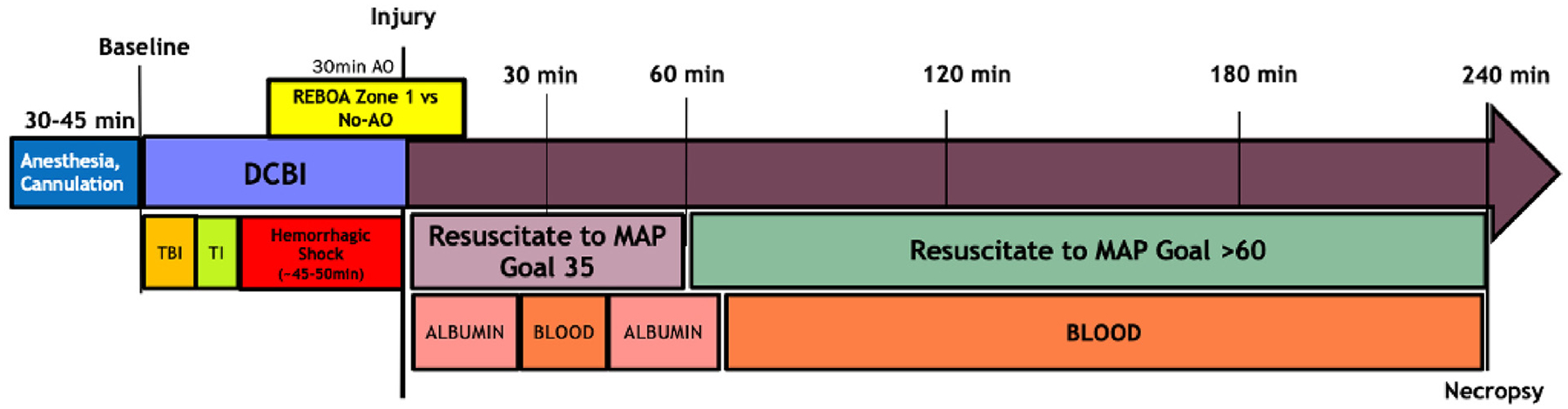
Methods: 50 kg male Yorkshire swine were subjected to a combination dismounted complex blast injury model consisting of blast traumatic brain injury (50 psi, ARA Mobile Shock Laboratory), tissue injury (bilateral femur fractures), and hemorrhagic shock (controlled bleeding to a base deficit goal of 10 mEq/L). During the shock phase, pigs were randomized to no aortic occlusion (n = 8) or to 30 minutes of zone 1 resuscitative endovascular balloon occlusion of the aorta (zone 1 aortic occlusion group, n = 6). After shock, pigs in both groups received a modified Tactical Combat Casualty Care-based resuscitation and were monitored for an additional 240 minutes until euthanasia/death for a total of 6 hours. Intracranial pressure was monitored throughout, and brains were harvested for water content. Linear mixed models for repeated measures were used to compare mean arterial pressure and intracranial pressure between zone 1 aortic occlusion and no aortic occlusion groups.
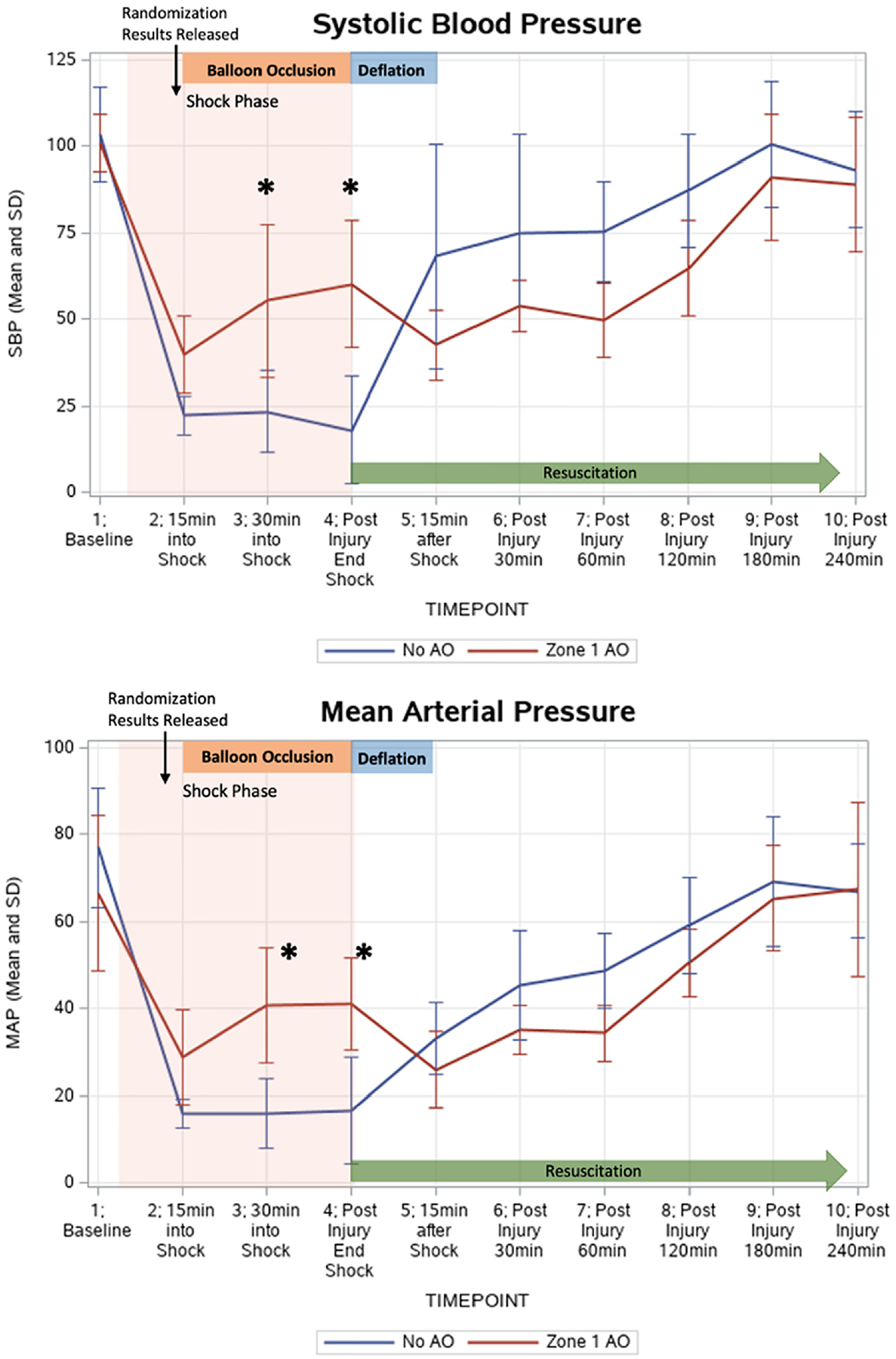
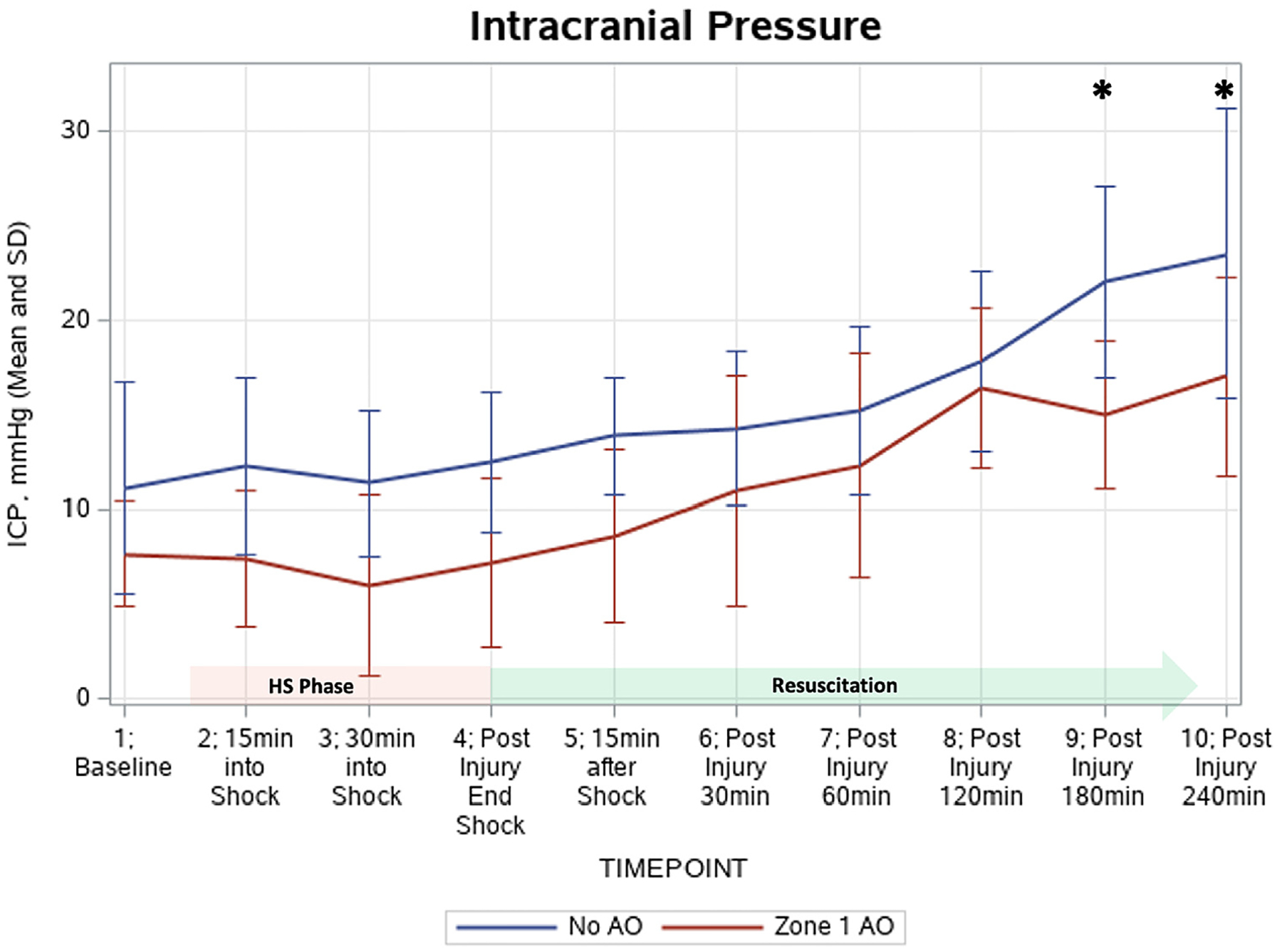
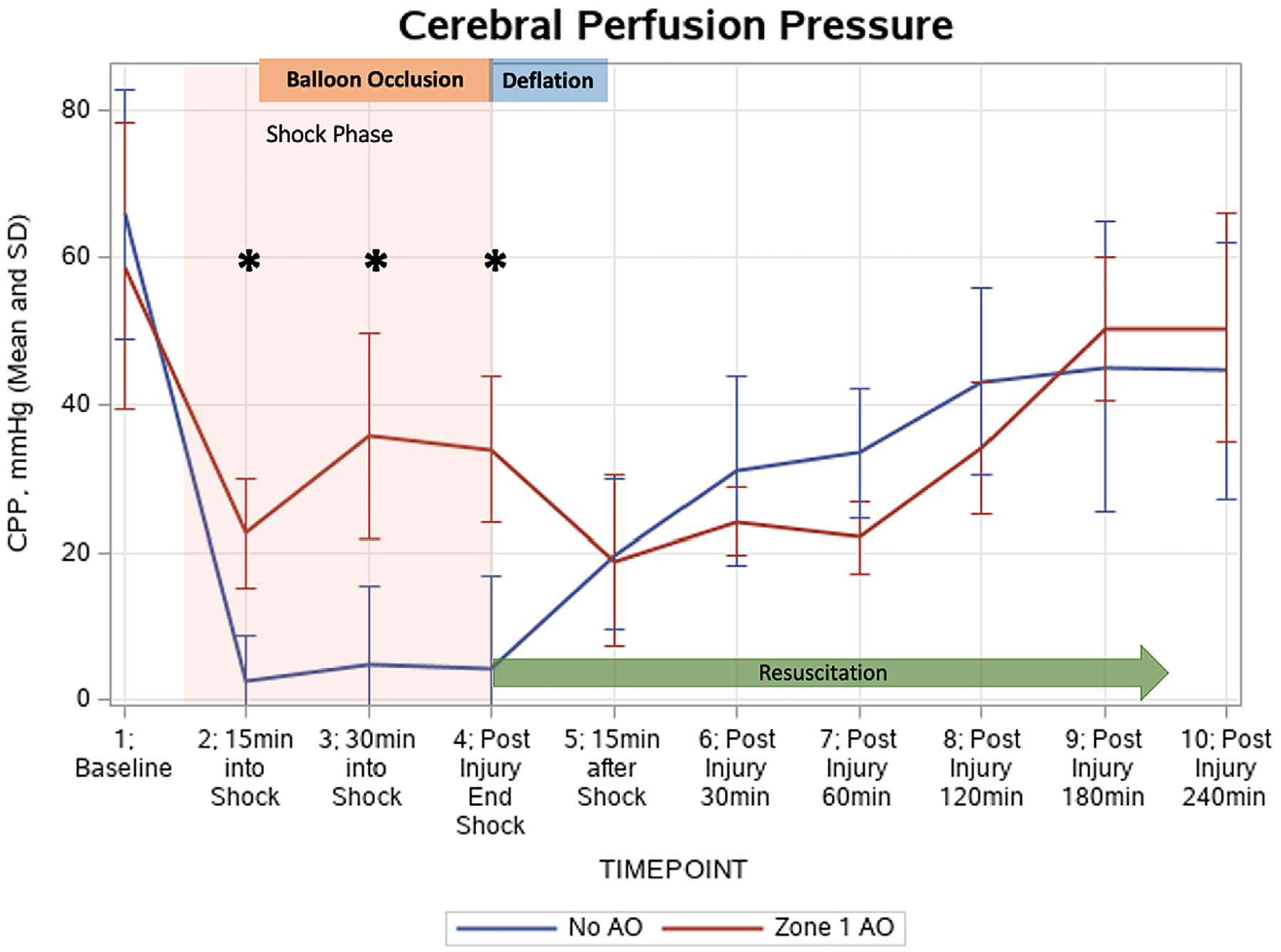
Results: After dismounted complex blast injury, the zone 1 group had a significantly higher mean arterial pressure during hemorrhagic shock compared to the control group (41.2 mm Hg vs 16.7 mm Hg, P = .002). During balloon occlusion, intracranial pressure was not significantly elevated in the zone 1 aortic occlusion group vs control, but intracranial pressure was significantly lower in the zone 1 group at the end of the observation period. In addition, the zone 1 aortic occlusion group did not have increased brain water content (zone 1 aortic occlusion: 3.95 ± 0.1g vs no aortic occlusion: 3.95 ± 0.3 g, P = .87). Troponin levels significantly increased in the no aortic occlusion group but did not in the zone 1 aortic occlusion group.
Conclusion: Zone 1 aortic occlusion using resuscitative endovascular balloon occlusion of the aorta in a large animal dismounted complex blast injury model improved proximal mean arterial pressure while not significantly increasing intracranial pressure during balloon inflation. Observation up to 240 minutes postresuscitation did not show clinical signs of worsening brain injury or cardiac injury. These data suggest that in a dismounted complex blast injury swine model, resuscitative endovascular balloon occlusion of the aorta in zone 1 may provide neuro- and cardioprotection in the setting of blast traumatic brain injury. However, longer monitoring periods may be needed to confirm that the neuroprotection is lasting.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
-
- Rhee P, Joseph B, Pandit V, et al. Increasing trauma deaths in the United States. Ann Surg. 2014;260:13–21. - PubMed
-
- Morrison JJ, Ross JD, Rasmussen TE, Midwinter MJ, Jansen JO. Resuscitative endovascular balloon occlusion of the aorta: a gap analysis of severely injured UK combat casualties. Shock. 2014;41:388–393. - PubMed
-
- Cannon JW, Hofmann LJ, Glasgow SC, et al. Dismounted complex blast injuries: a comprehensive review of the modern combat experience. J Am Coll Surg. 2016;223:652–664.e8. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001–2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S431–S437. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
