

Mechanical loading of cranial joints minimizes the craniofacial phenotype in Crouzon syndrome
- PMID: 35690633
- PMCID: PMC9188582
- DOI: 10.1038/s41598-022-13807-9
Mechanical loading of cranial joints minimizes the craniofacial phenotype in Crouzon syndrome
Abstract
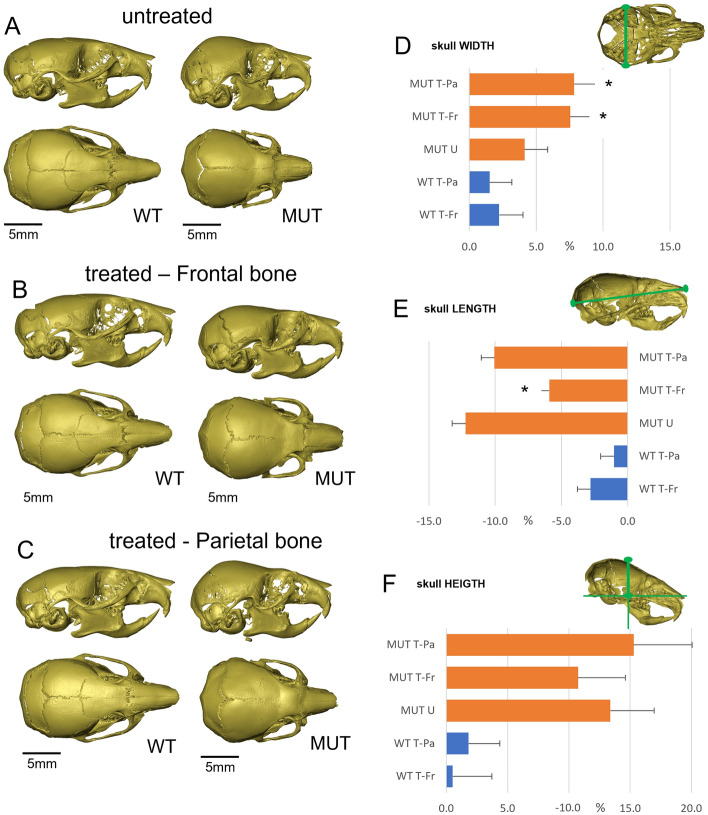
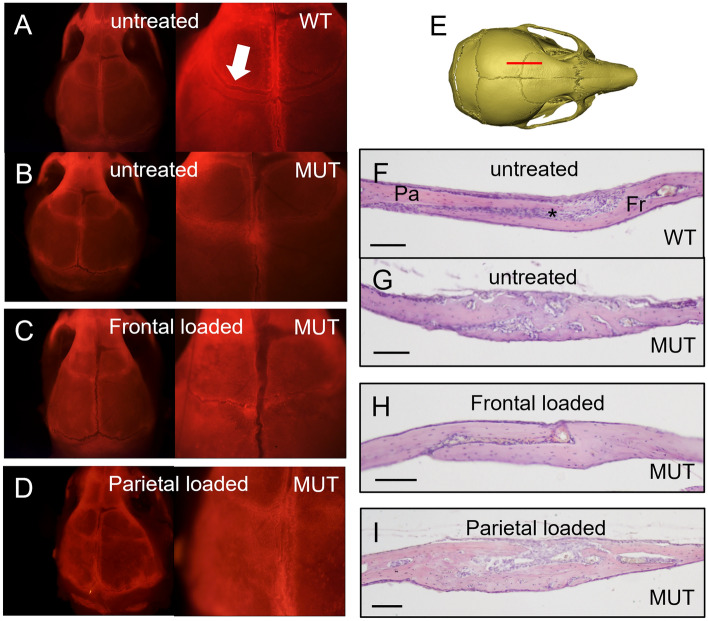
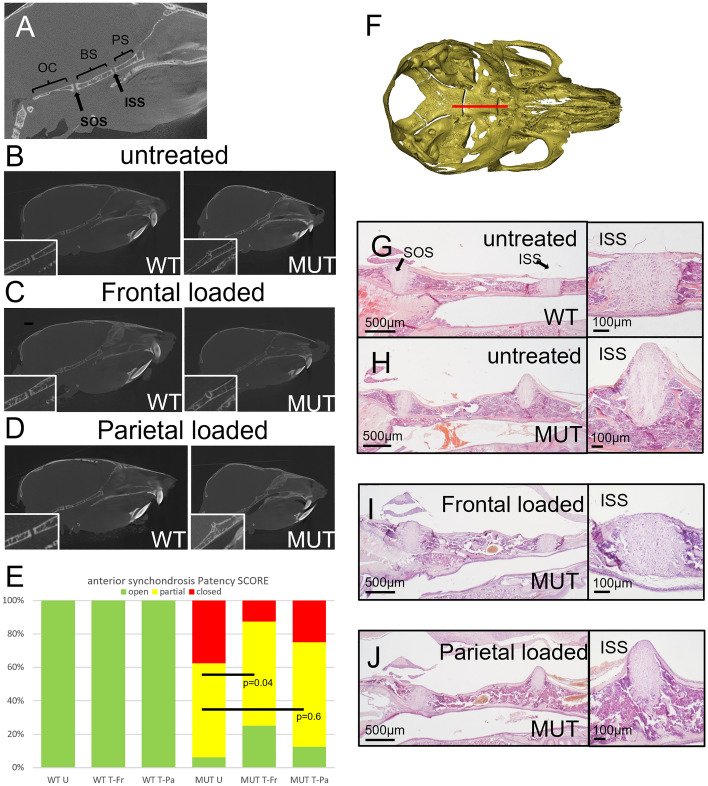
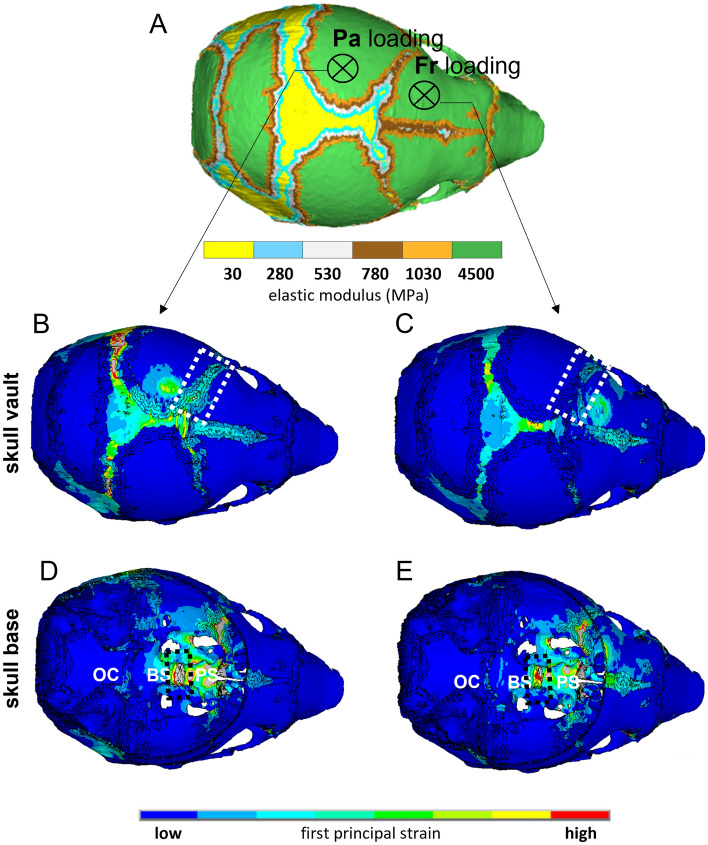
Children with syndromic forms of craniosynostosis undergo a plethora of surgical interventions to resolve the clinical features caused by the premature fusion of cranial sutures. While surgical correction is reliable, the need for repeated rounds of invasive treatment puts a heavy burden on the child and their family. This study explores a non-surgical alternative using mechanical loading of the cranial joints to prevent or delay craniofacial phenotypes associated with Crouzon syndrome. We treated Crouzon syndrome mice before the onset of craniosynostosis by cyclical mechanical loading of cranial joints using a custom designed set-up. Cranial loading applied to the frontal bone partially restores normal skull morphology, significantly reducing the typical brachycephalic appearance. This is underpinned by the delayed closure of the coronal suture and of the intersphenoidal synchondrosis. This study provides a novel treatment alternative for syndromic craniosynostosis which has the potential to be an important step towards replacing, reducing or refining the surgical treatment of all craniosynostosis patients.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- EUROCAT. European Platform on Rare Disease Registration-Prevalence. https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en (2021).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
