

Vagus nerve stimulation does not improve recovery of forelimb motor or somatosensory function in a model of neuropathic pain
- PMID: 35690673
- PMCID: PMC9188565
- DOI: 10.1038/s41598-022-13621-3
Vagus nerve stimulation does not improve recovery of forelimb motor or somatosensory function in a model of neuropathic pain
Abstract
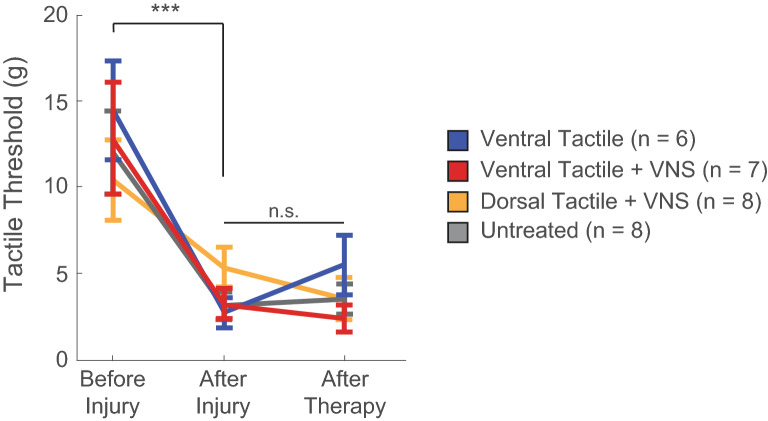
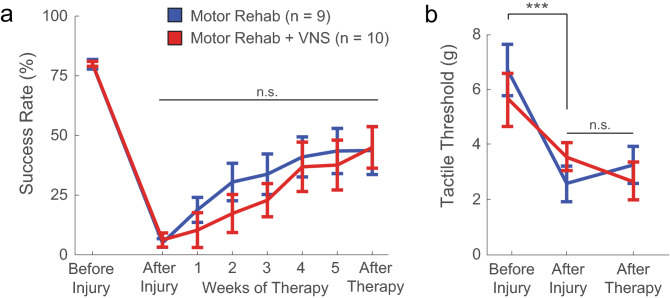
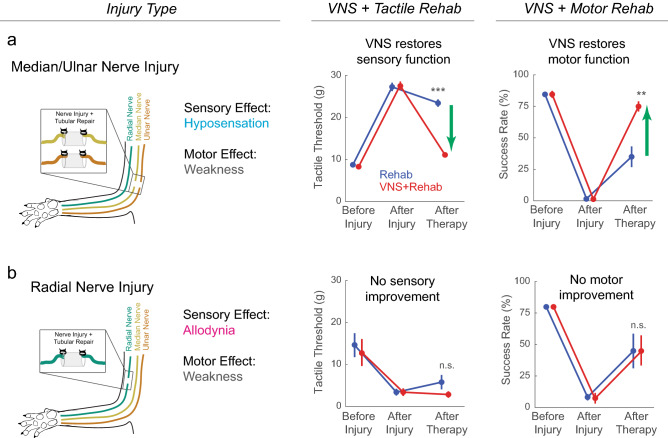
Nerve injury affecting the upper limb is a leading cause of lifelong disability. Damage to the nerves in the arm often causes weakness and somatosensory dysfunction ranging from numbness to pain. Previous studies show that combining brief bursts of electrical vagus nerve stimulation (VNS) with motor or tactile rehabilitation can restore forelimb function after median and ulnar nerve injury, which causes hyposensitivity of the ventral forelimb. Here, we sought to determine whether this approach would be similarly effective in a model of radial nerve injury that produces allodynia in the ventral forelimb. To test this, rats underwent complete transection of the radial nerve proximal to the elbow followed by tubular repair. In the first experiment, beginning ten weeks after injury, rats received six weeks of tactile rehabilitation, consisting of mechanical stimulation of either the dorsal or ventral region of the forepaw in the injured limb, with or without concurrent VNS. In a second experiment, a separate cohort of rats underwent six weeks of forelimb motor rehabilitative training with or without paired VNS. Contrary to findings in previous models of hyposensitivity, VNS therapy fails to improve recovery of either somatosensory or motor function in the forelimb after radial nerve injury. These findings describe initial evidence that pain may limit the efficacy of VNS therapy and thus highlight a characteristic that should be considered in future studies that seek to develop this intervention.
© 2022. The Author(s).
Conflict of interest statement
MPK is a consultant for and shareholder in MicroTransponder, which is developing VNS for stroke. RLR is CEO of XNerve, which is developing VNS technology. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
