

An electronic health record (EHR) phenotype algorithm to identify patients with attention deficit hyperactivity disorders (ADHD) and psychiatric comorbidities
- PMID: 35690720
- PMCID: PMC9188139
- DOI: 10.1186/s11689-022-09447-9
An electronic health record (EHR) phenotype algorithm to identify patients with attention deficit hyperactivity disorders (ADHD) and psychiatric comorbidities
Abstract
Background: In over half of pediatric cases, ADHD presents with comorbidities, and often, it is unclear whether the symptoms causing impairment are due to the comorbidity or the underlying ADHD. Comorbid conditions increase the likelihood for a more severe and persistent course and complicate treatment decisions. Therefore, it is highly important to establish an algorithm that identifies ADHD and comorbidities in order to improve research on ADHD using biorepository and other electronic record data.
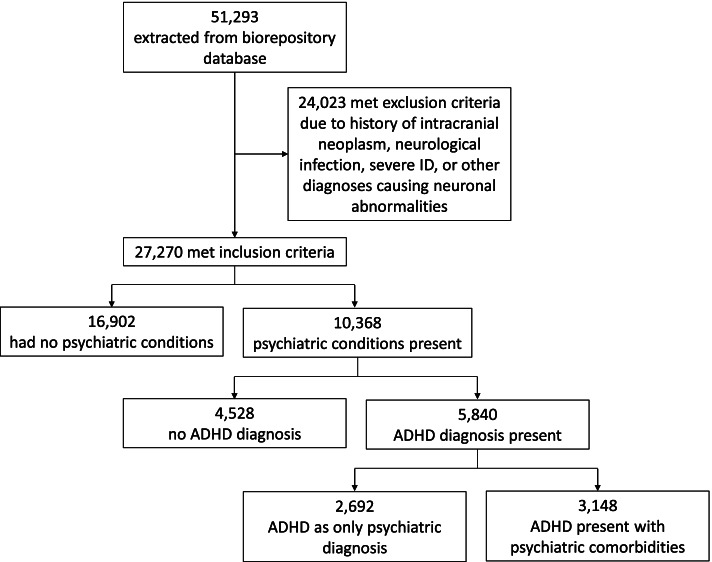
Methods: It is feasible to accurately distinguish between ADHD in isolation from ADHD with comorbidities using an electronic algorithm designed to include other psychiatric disorders. We sought to develop an EHR phenotype algorithm to discriminate cases with ADHD in isolation from cases with ADHD with comorbidities more effectively for efficient future searches in large biorepositories. We developed a multi-source algorithm allowing for a more complete view of the patient's EHR, leveraging the biobank of the Center for Applied Genomics (CAG) at Children's Hospital of Philadelphia (CHOP). We mined EHRs from 2009 to 2016 using International Statistical Classification of Diseases and Related Health Problems (ICD) codes, medication history and keywords specific to ADHD, and comorbid psychiatric disorders to facilitate genotype-phenotype correlation efforts. Chart abstractions and behavioral surveys added evidence in support of the psychiatric diagnoses. Most notably, the algorithm did not exclude other psychiatric disorders, as is the case in many previous algorithms. Controls lacked psychiatric and other neurological disorders. Participants enrolled in various CAG studies at CHOP and completed a broad informed consent, including consent for prospective analyses of EHRs. We created and validated an EHR-based algorithm to classify ADHD and comorbid psychiatric status in a pediatric healthcare network to be used in future genetic analyses and discovery-based studies.
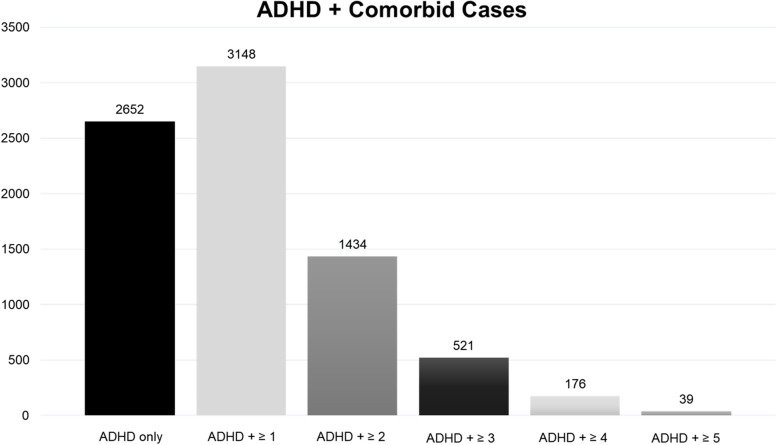
Results: In this retrospective case-control study that included data from 51,293 subjects, 5840 ADHD cases were discovered of which 46.1% had ADHD alone and 53.9% had ADHD with psychiatric comorbidities. Our primary study outcome was to examine whether the algorithm could identify and distinguish ADHD exclusive cases from ADHD comorbid cases. The results indicate ICD codes coupled with medication searches revealed the most cases. We discovered ADHD-related keywords did not increase yield. However, we found including ADHD-specific medications increased our number of cases by 21%. Positive predictive values (PPVs) were 95% for ADHD cases and 93% for controls.
Conclusion: We established a new algorithm and demonstrated the feasibility of the electronic algorithm approach to accurately diagnose ADHD and comorbid conditions, verifying the efficiency of our large biorepository for further genetic discovery-based analyses.
Trial registration: ClinicalTrials.gov, NCT02286817 . First posted on 10 November 2014.
Clinicaltrials: gov, NCT02777931 . First posted on 19 May 2016.
Clinicaltrials: gov, NCT03006367 . First posted on 30 December 2016.
Clinicaltrials: gov, NCT02895906 . First posted on 12 September 2016.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
