

Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: a cohort study in claims databases
- PMID: 35691322
- PMCID: PMC9183215
- DOI: 10.1016/S0140-6736(22)00791-7
Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: a cohort study in claims databases
Abstract
Background: Several passive surveillance systems reported increased risks of myocarditis or pericarditis, or both, after COVID-19 mRNA vaccination, especially in young men. We used active surveillance from large health-care databases to quantify and enable the direct comparison of the risk of myocarditis or pericarditis, or both, after mRNA-1273 (Moderna) and BNT162b2 (Pfizer-BioNTech) vaccinations.
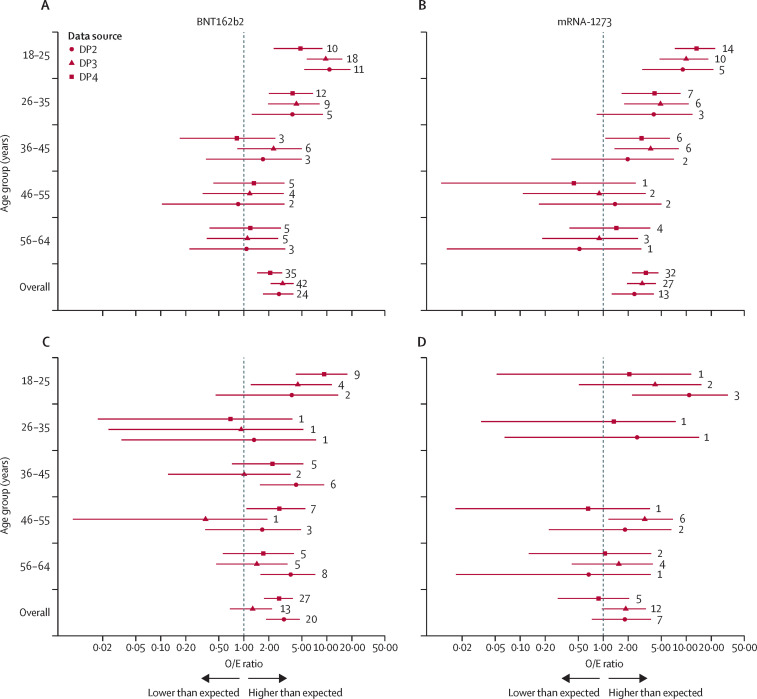
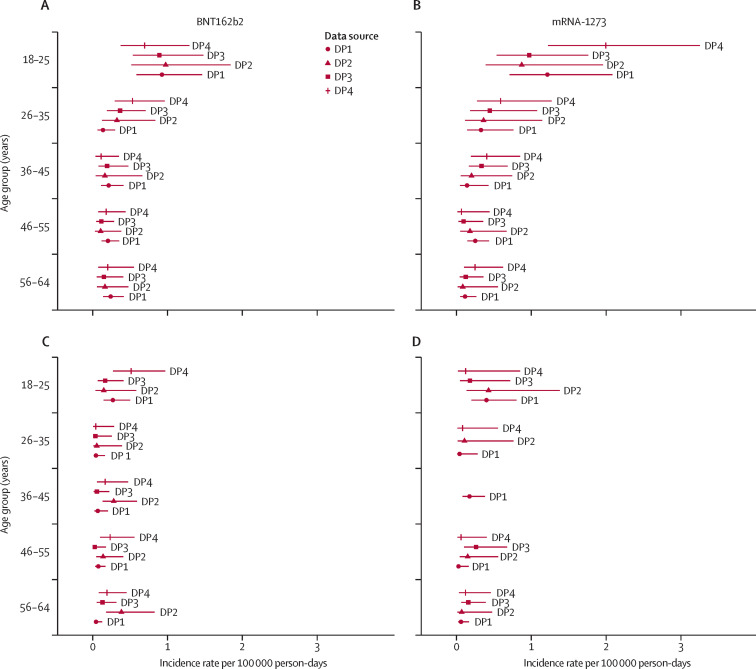
Methods: We conducted a retrospective cohort study, examining the primary outcome of myocarditis or pericarditis, or both, identified using the International Classification of Diseases diagnosis codes, occurring 1-7 days post-vaccination, evaluated in COVID-19 mRNA vaccinees aged 18-64 years using health plan claims databases in the USA. Observed (O) incidence rates were compared with expected (E) incidence rates estimated from historical cohorts by each database. We used multivariate Poisson regression to estimate the adjusted incidence rates, specific to each brand of vaccine, and incidence rate ratios (IRRs) comparing mRNA-1273 and BNT162b2. We used meta-analyses to pool the adjusted incidence rates and IRRs across databases.
Findings: A total of 411 myocarditis or pericarditis, or both, events were observed among 15 148 369 people aged 18-64 years who received 16 912 716 doses of BNT162b2 and 10 631 554 doses of mRNA-1273. Among men aged 18-25 years, the pooled incidence rate was highest after the second dose, at 1·71 (95% CI 1·31 to 2·23) per 100 000 person-days for BNT162b2 and 2·17 (1·55 to 3·04) per 100 000 person-days for mRNA-1273. The pooled IRR in the head-to-head comparison of the two mRNA vaccines was 1·43 (95% CI 0·88 to 2·34), with an excess risk of 27·80 per million doses (-21·88 to 77·48) in mRNA-1273 recipients compared with BNT162b2.
Interpretation: An increased risk of myocarditis or pericarditis was observed after COVID-19 mRNA vaccination and was highest in men aged 18-25 years after a second dose of the vaccine. However, the incidence was rare. These results do not indicate a statistically significant risk difference between mRNA-1273 and BNT162b2, but it should not be ruled out that a difference might exist. Our study results, along with the benefit-risk profile, continue to support vaccination using either of the two mRNA vaccines.
Funding: US Food and Drug Administration.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests All Optum Epidemiology coauthors are employees of Optum. KLA and JDS own stock in UnitedHealth Group. All other authors declare no competing interests.
Figures
Comment in
-
COVID-19 mRNA vaccination and myocarditis or pericarditis.Lancet. 2022 Jun 11;399(10342):2168-2169. doi: 10.1016/S0140-6736(22)00842-X. Lancet. 2022. PMID: 35691306 Free PMC article. No abstract available.
References
-
- European Medicines Authority Signal assessment report on myocarditis and pericarditis with Spikevax (previously COVID-19 Vaccine Moderna) 2021. https://www.ema.europa.eu/en/documents/prac-recommendation/signal-assess...
-
- Public Health Ontario Adverse events following immunization (AEFI) for COVID-19 in Ontario: December 13, 2020 to October 10, 2021. 2021. https://www.publichealthontario.ca/-/media/documents/ncov/epi/covid-19-a...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
