

Association between choice of reversal agent for neuromuscular block and postoperative pulmonary complications in patients at increased risk undergoing non-emergency surgery: STIL-STRONGER, a multicentre matched cohort study
- PMID: 35691703
- PMCID: PMC9875908
- DOI: 10.1016/j.bja.2022.04.023
Association between choice of reversal agent for neuromuscular block and postoperative pulmonary complications in patients at increased risk undergoing non-emergency surgery: STIL-STRONGER, a multicentre matched cohort study
Abstract
Background: Postoperative pulmonary complications are a source of morbidity after major surgery. In patients at increased risk of postoperative pulmonary complications we sought to assess the association between neuromuscular blocking agent reversal agent and development of postoperative pulmonary complications.
Methods: We conducted a retrospective matched cohort study, a secondary analysis of data collected in the prior STRONGER study. Data were obtained from the Multicenter Perioperative Outcomes Group. Included patients were aged 18 yr and older undergoing non-emergency surgery under general anaesthesia with tracheal intubation with neuromuscular block and reversal, who were predicted to be at elevated risk of postoperative pulmonary complications. This risk was defined as American Society of Anesthesiologists Physical Status 3 or 4 in patients undergoing either intrathoracic or intra-abdominal surgery who were either aged >80 yr or underwent a procedure lasting >2 h. Cohorts were defined by reversal with neostigmine or sugammadex. The primary composite outcome was the occurrence of pneumonia or respiratory failure.
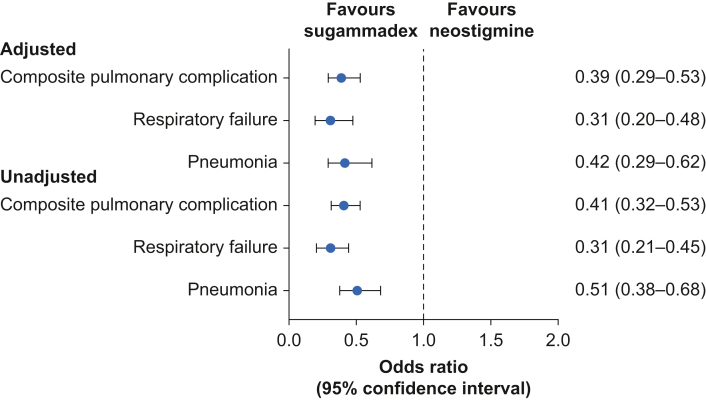
Results: After matching by institution, sex, age (within 5 yr), body mass index, anatomic region of surgery, comorbidities, and neuromuscular blocking agent, 3817 matched pairs remained. The primary postoperative pulmonary complications outcome occurred in 224 neostigmine cases vs 100 sugammadex cases (5.9% vs 2.6%, odds ratio 0.41, P<0.01). After adjustment for unbalanced covariates, the adjusted odds ratio for the association between sugammadex use and the primary outcome was 0.39 (P<0.0001).
Conclusions: In a cohort of patients at increased risk for pulmonary complications compared with neostigmine, use of sugammadex was independently associated with reduced risk of subsequent development of pneumonia or respiratory failure.
Keywords: neostigmine; neuromuscular blocking drug; pneumonia; postoperative pulmonary complications; respiratory failure; reversal of neuromuscular block; sugammadex.
Copyright © 2022 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures

Comment in
-
How robust are the STRONGER and STIL-STRONGER studies?Br J Anaesth. 2023 Jan;130(1):e41-e44. doi: 10.1016/j.bja.2022.08.021. Epub 2022 Sep 29. Br J Anaesth. 2023. PMID: 36182557
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
