

Osteoporosis in 2022: Care gaps to screening and personalised medicine
- PMID: 35691824
- PMCID: PMC7614114
- DOI: 10.1016/j.berh.2022.101754
Osteoporosis in 2022: Care gaps to screening and personalised medicine
Abstract
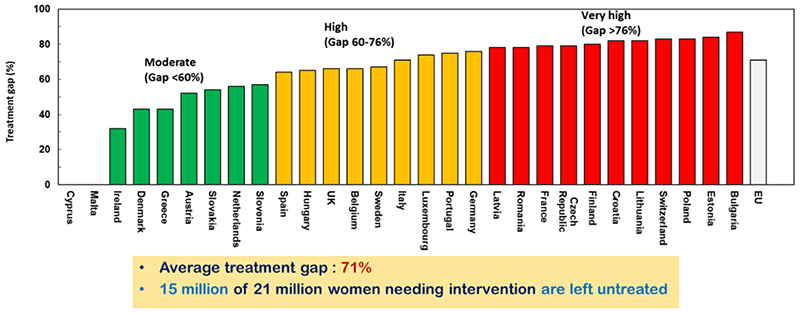
Osteoporosis care has evolved markedly over the last 50 years, such that there are now an established clinical definition, validated methods of fracture risk assessment, and a range of effective pharmacological agents. However, it is apparent that both in the context of primary and secondary fracture prevention, there is a considerable gap between the population at high fracture risk and those actually receiving appropriate antiosteoporosis treatment. In this narrative review article, we document recent work describing the burden of disease, approaches to management, and service provision across Europe, emerging data on gaps in care, and existing/new ways in which these gaps may be addressed at the level of healthcare systems and policy. We conclude that although the field has come a long way in recent decades, there is still a long way to go, and a concerted, integrated effort is now required from all of us involved in this field to address these urgent issues to ensure the best possible outcomes for our patients.
Keywords: Epidemiology; Fracture; Osteoporosis; Policy; Treatment gap.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest EC reports honoraria/travel support from Eli Lilly, UCB and Amgen outside the submitted work. EMD reports no conflicts of interest. CC reports personal fees from ABBH, Amgen, Eli Lilly, GSK, Medtronic, Merck, Novartis, Pfizer, Roche, Servier and Takeda, outside the submitted work. NCH reports personal fees, consultancy, lecture fees and honoraria from Alliance for Better Bone Health, AMGEN, MSD, Eli Lilly, Servier, Shire, Consilient Healthcare, UCB, Kyowa Kirin and Internis Pharma, outside the submitted work.
Figures
References
-
- Harvey NC, McCloskey E. Gaps and solutions in bone health: A global framework for improvement. 2016.
Publication types
MeSH terms
Grants and funding
- 17702/VAC_/Versus Arthritis/United Kingdom
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- 21231/VAC_/Versus Arthritis/United Kingdom
- MC_PC_21003/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_PC_21001/MRC_/Medical Research Council/United Kingdom
- 19583/VAC_/Versus Arthritis/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MC_PC_21022/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_PC_21000/MRC_/Medical Research Council/United Kingdom
- MRF-145-0011-DG-HARV-C0913/MRF_/MRF_/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- 10/33/04/DH_/Department of Health/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
