

The Effects of Different Anesthesia Methods on the Treatment of Parkinson's Disease by Bilateral Deep Brain Stimulation of the Subthalamic Nucleus
- PMID: 35692425
- PMCID: PMC9178204
- DOI: 10.3389/fnins.2022.917752
The Effects of Different Anesthesia Methods on the Treatment of Parkinson's Disease by Bilateral Deep Brain Stimulation of the Subthalamic Nucleus
Abstract
Background: Subthalamic nucleus deep brain stimulation (STN-DBS) surgery for Parkinson's disease (PD) is routinely performed at medical centers worldwide. However, it is debated whether general anesthesia (GA) or traditional local anesthetic (LA) is superior.
Purpose: This study aims to compare the effects of LA and GA operation methods on clinical improvement in patients with PD, such as motor and non-motor symptoms, after STN-DBS surgery at our center.
Method: A total of 157 patients with PD were retrospectively identified as having undergone surgery under LA (n = 81) or GA (n = 76) states. In this study, the Unified Parkinson's Disease Rating Scale Motor Score (UPDRS-III) in three states, levodopa-equivalent-daily-dose (LEDD), surgical duration, intraoperative microelectrode recording (iMER) signal length, postoperative intracranial volume, electrode implantation error, neuropsychological function, quality of life scores, and complication rates were collected and compared. All patients with PD were routinely followed up at 6, 12, 18, and 24 months postoperatively.
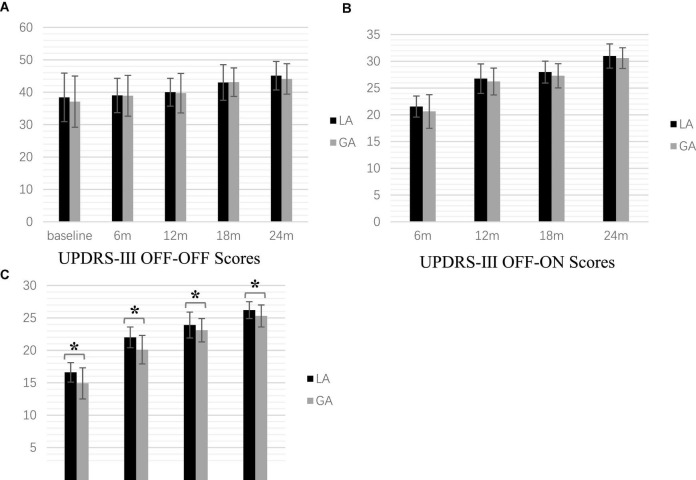
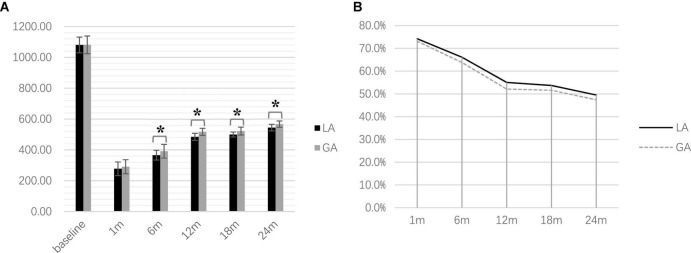
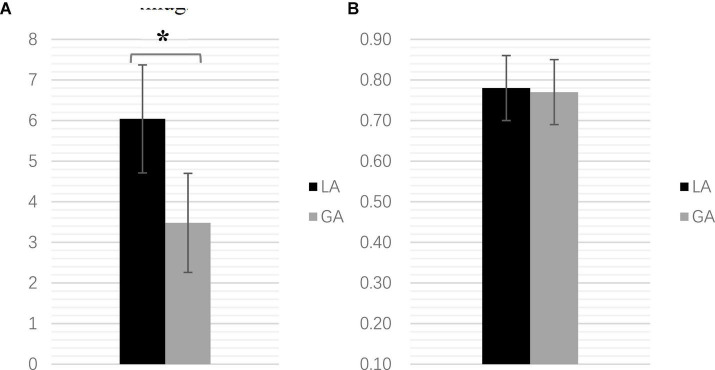
Result: Overall improvement in UPDRS-III was demonstrated at postoperative follow-up, and there was no significant difference between the two groups in medication-off, stimulation-off state and medication-off, stimulation-on state. However, UPDRS-III scores in medication-on, stimulation-on state under GA was significantly lower than that in the LA group. During postoperative follow-up, LEDD in the LA group (6, 12, 18, and 24 months, postoperatively) was significantly lower than in the GA group. However, there were no significant differences at baseline or 1-month between the two groups. The GA group had a shorter surgical duration, lower intracranial volume, and longer iMER signal length than the LA group. However, there was no significant group difference in electrode implantation accuracy and complication rates. Additionally, the Hamilton Anxiety Scale (HAMA) was significantly lower in the GA group than the LA group at 1-month follow-up, but this difference disappeared at longer follow-up. Besides, there was no significant group difference in the 39-item Parkinson's Disease Questionnaire (PDQ-39) scale scores.
Conclusion: Although both groups showed overall motor function improvement without a significant postoperative difference, the GA group seemed superior in surgical duration, intracranial volume, and iMER signal length. As the accuracy of electrode implantation can be ensured by iMER monitoring, DBS with GA will become more widely accepted.
Keywords: Parkinson’s disease; deep brain stimulation; general anesthesia; intraoperative microelectrode recording; local anesthesia; subthalamic nucleus.
Copyright © 2022 Lu, Chang, Li, Luo, Dong, Qiu, Zhang and Ruan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bezchlibnyk Y. B., Sharma V. D., Naik K. B., Isbaine F., Gale J. T., Cheng J., et al. (2020). Clinical outcomes of globus pallidus deep brain stimulation for Parkinson disease: a comparison of intraoperative MRI- and MER-guided lead placement. J. Neurosurg. 134 1072–1082. 10.3171/2019.12.JNS192010 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials