

The Time Course of Quadriceps Strength Recovery After Total Knee Arthroplasty Is Influenced by Body Mass Index, Sex, and Age of Patients: Systematic Review and Meta-Analysis
- PMID: 35692543
- PMCID: PMC9174520
- DOI: 10.3389/fmed.2022.865412
The Time Course of Quadriceps Strength Recovery After Total Knee Arthroplasty Is Influenced by Body Mass Index, Sex, and Age of Patients: Systematic Review and Meta-Analysis
Abstract
Introduction: For patients with osteoarthritis who have undergone total knee arthroplasty (TKA), quadriceps strength is a major determinant of general physical function regardless of the parameters adopted for functional assessment. Understanding the time course of quadriceps strength recovery and effectiveness of different rehabilitation protocols is a must. Therefore, the aim of this study was to: (i) determine the magnitude of maximal voluntary strength (MVS) loss and the time course of recovery of the quadriceps muscle following TKA, (ii) identify potential moderators of strength outcomes, and (iii) investigate whether different rehabilitation practices can moderate the strength outcomes following TKA, respectively.
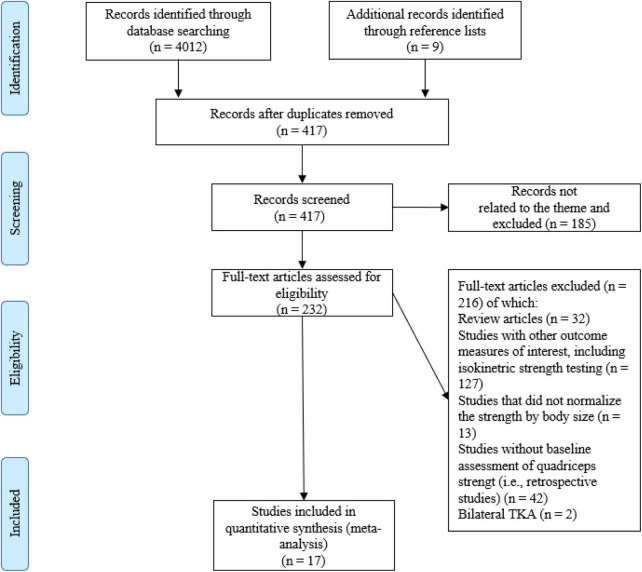
Design: General scientific databases and relevant journals in the field of orthopedics were searched, identifying prospective studies that investigated quadriceps' MVS pre-to post-surgery.
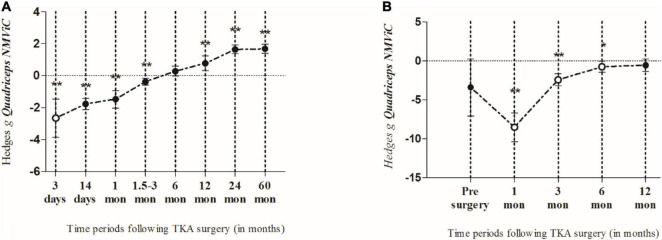
Results: Seventeen studies with a total of 832 patients (39% males) were included. Results showed that in the early post-operative days, the involved quadriceps' MVS markedly declined, after which it slowly recovered over time in a linear fashion. Thus, the greatest decline of the MVS was observed 3 days after TKA. When compared to pre-operative values, the MVS was still significantly lower 3 months after TKA and did not fully recover up to 6 months following TKA. Furthermore, a meta-regression analysis identified that the variables, time point of evaluation, patient age, sex, and BMI, significantly moderate the MVS of the quadriceps muscle.
Conclusion: The analyzed literature data showed that the decrease in strength of the involved quadriceps muscles following TKA is considerable and lasts for several months post-surgery. Therefore, we recommend to specifically target the strengthening of knee extensor muscles, preserve motor control, and apply appropriate nutrition to ensure a holistic quadriceps muscle recovery. Since age, sex, and BMI were found to be moderating factors in patients' recovery, further research should include specific analyses considering these moderators.
Keywords: body mass index (BMI); functional performance; knee osteoarthritis; rehabilitation; total knee replacement; voluntary activation.
Copyright © 2022 Paravlic, Meulenberg and Drole.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Neurostructural correlates of strength decrease following total knee arthroplasty: A systematic review of the literature with meta-analysis.Bosn J Basic Med Sci. 2020 Feb 5;20(1):1-12. doi: 10.17305/bjbms.2019.3814. Bosn J Basic Med Sci. 2020. PMID: 30640590 Free PMC article.
-
Quadriceps/hamstrings co-activation increases early after total knee arthroplasty.Knee. 2014 Dec;21(6):1115-9. doi: 10.1016/j.knee.2014.08.001. Epub 2014 Sep 11. Knee. 2014. PMID: 25218971 Free PMC article.
-
Quadriceps strength and the time course of functional recovery after total knee arthroplasty.J Orthop Sports Phys Ther. 2005 Jul;35(7):424-36. doi: 10.2519/jospt.2005.35.7.424. J Orthop Sports Phys Ther. 2005. PMID: 16108583
-
Improvement in hamstring and quadriceps muscle strength following cruciate-retaining single radius total knee arthroplasty.Ann Transl Med. 2017 Dec;5(Suppl 3):S27. doi: 10.21037/atm.2017.11.14. Ann Transl Med. 2017. PMID: 29299474 Free PMC article.
-
The relationship between prescribed pre-operative knee-extensor exercise dosage and effect on knee-extensor strength prior to and following total knee arthroplasty: a systematic review and meta-regression analysis of randomized controlled trials.Osteoarthritis Cartilage. 2020 Nov;28(11):1412-1426. doi: 10.1016/j.joca.2020.08.011. Epub 2020 Sep 2. Osteoarthritis Cartilage. 2020. PMID: 32890744
Cited by
-
What Influences Patients Readiness for Discharge: The Case of Total Knee Arthroplasty: A Cross-Sectional Study.J Nurs Manag. 2024 Apr 1;2024:8032254. doi: 10.1155/2024/8032254. eCollection 2024. J Nurs Manag. 2024. PMID: 40224761 Free PMC article.
-
Comparison of the Effects of Adductor Canal and Femoral Nerve Blocks on Postoperative Opioid Consumption and Inflammatory Factor Levels in Elderly Patients After Total Knee Arthroplasty: A Prospective Observational Study.J Pain Res. 2024 Jul 11;17:2375-2391. doi: 10.2147/JPR.S463097. eCollection 2024. J Pain Res. 2024. PMID: 39011277 Free PMC article.
-
Characterizing patient factors, perioperative interventions, and outcomes associated with inpatients falls after total knee arthroplasty.Knee Surg Relat Res. 2024 Mar 8;36(1):11. doi: 10.1186/s43019-024-00215-8. Knee Surg Relat Res. 2024. PMID: 38459532 Free PMC article.
-
The past and future of peri-operative interventions to reduce arthrogenic quadriceps muscle inhibition after total knee arthroplasty: A narrative review.Osteoarthr Cartil Open. 2023 Dec 21;6(1):100429. doi: 10.1016/j.ocarto.2023.100429. eCollection 2024 Mar. Osteoarthr Cartil Open. 2023. PMID: 38304413 Free PMC article. Review.
-
Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study.Healthcare (Basel). 2023 Jan 26;11(3):356. doi: 10.3390/healthcare11030356. Healthcare (Basel). 2023. PMID: 36766931 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources