

Surgical Strategies and Outcomes for Intracranial Chondromas: A Retrospective Study of 17 Cases and Systematic Review
- PMID: 35692788
- PMCID: PMC9178658
- DOI: 10.3389/fonc.2022.865865
Surgical Strategies and Outcomes for Intracranial Chondromas: A Retrospective Study of 17 Cases and Systematic Review
Abstract
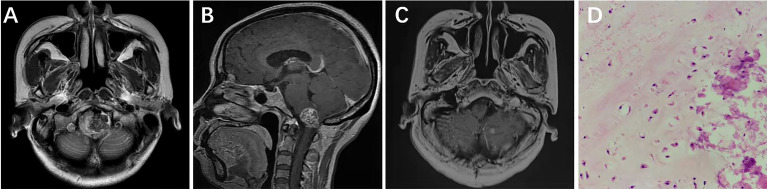
Objective: To improve the diagnosis and treatment of intracranial chondromas (ICDs) by discussing the clinical manifestations and imaging characteristics of ICDs, as well as surgical methods and treatment strategies.
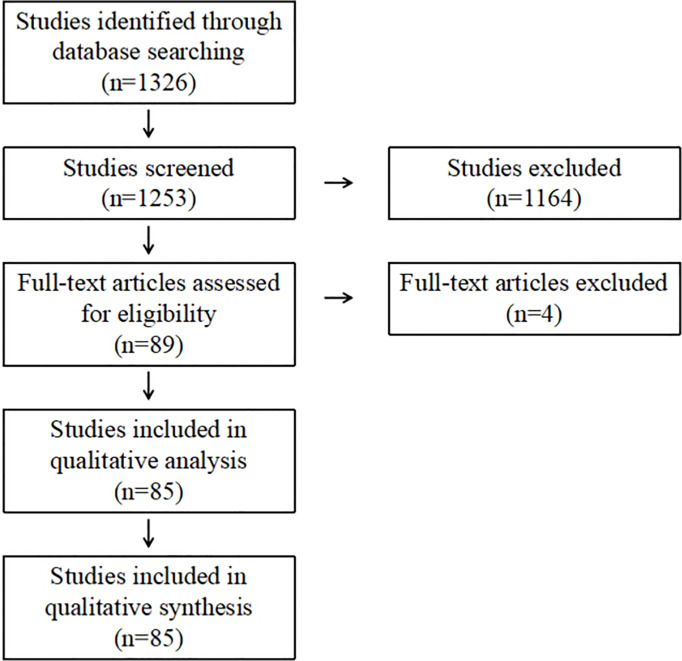
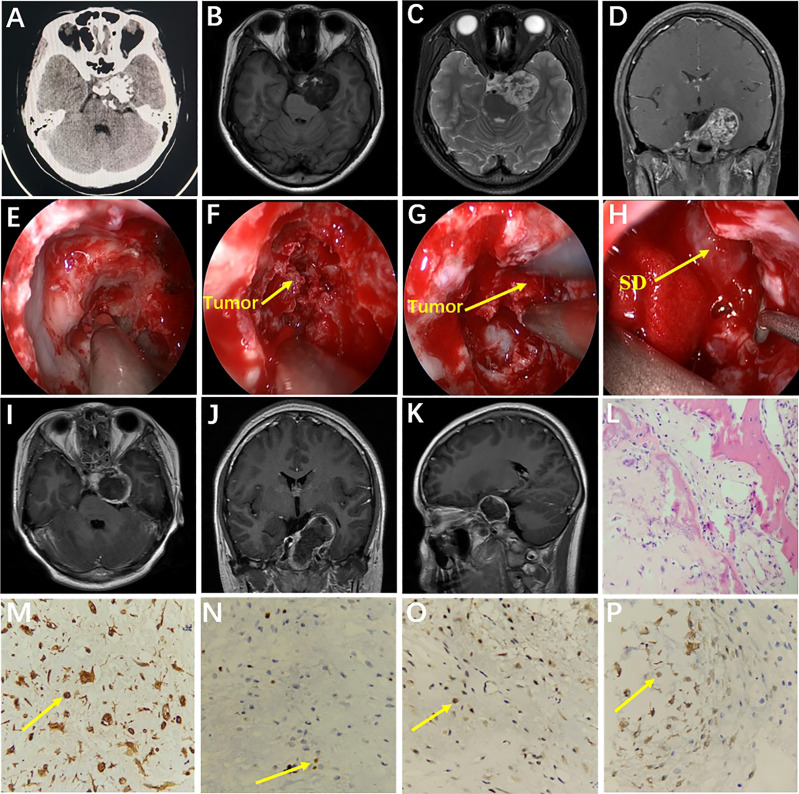
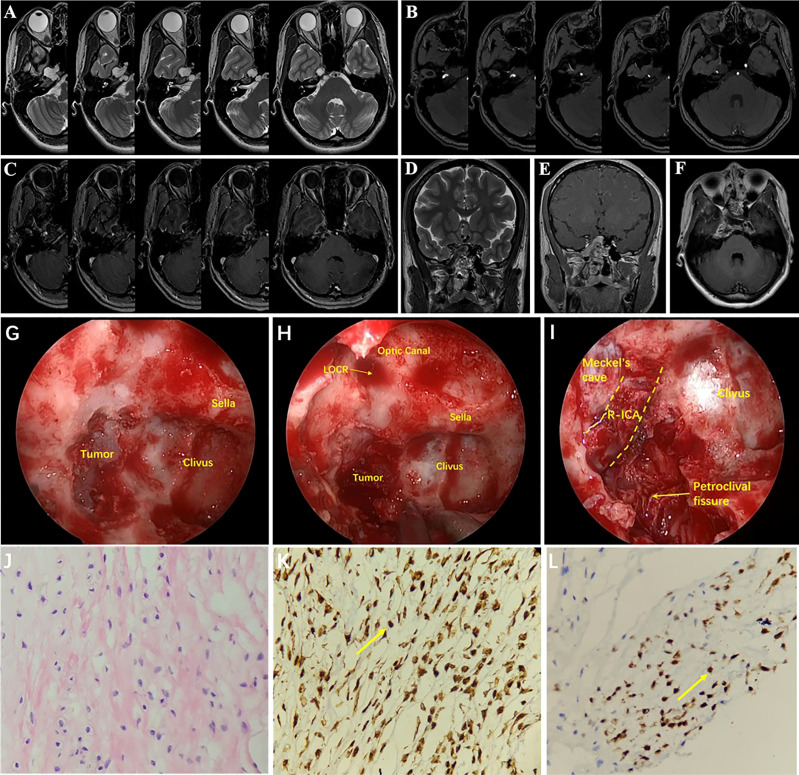
Methods: We retrospectively analyzed 17 patients diagnosed with ICDs who underwent microsurgery or endoscopic transsphenoidal surgery at the Tangdu Hospital of Air Force Military Medical University and the Mianyang Central Hospital from January 2010 to November 2021. Clinical manifestations, imaging examinations, surgical treatments, and prognosis of these patients were analyzed.
Results: ICDs had often been misdiagnosed as craniopharyngioma, chordoma, schwannoma, cavernous hemangioma, pituitary adenoma, and meningioma before surgery. Of the 17 cases, gross total resection (GTR) was performed in 10 cases, subtotal resection (STR) in 5, and partial resection in 2. GTR of tumor was achieved in eight cases via the endoscopic endonasal transsphenoidal approach (EETA) or the extended endoscopic endonasal transsphenoidal approach (EEETA), and the remaining patients underwent craniotomies. Clinical symptoms were assessed 1 week after surgery, 10 cases were relieved at varying degrees, and four cases had no improvement. Postoperative complications included right-limb hemiparesis, diplopia, eyelid ptosis, pulmonary infection, subcutaneous hydrops, cerebrospinal-fluid leakage (CSFL), and intracranial infection (ICI). One patient received gamma knife treatment at 3 months after surgery, two patients died due to tumor progression, and the remaining patients had no tumor recurrence.
Conclusions: ICDs lack typical imaging features and are often misdiagnosed. The EETA or EEETA helps improve the surgical outcomes and GTR rates of ICDs at different sites.
Keywords: endoscopic endonasal transsphenoidal approach; imaging features; intracranial chondromas; prognosis; surgical approach.
Copyright © 2022 Liu, Cai, Li, Xue, Zhang, Li, Zhao and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A multicenter retrospective analysis of clinical outcomes of intracranial chondrosarcoma in 26 patients.Sci Rep. 2023 Sep 5;13(1):14647. doi: 10.1038/s41598-023-41378-w. Sci Rep. 2023. PMID: 37669996 Free PMC article.
-
Therapeutic outcomes of transsphenoidal surgery in pediatric patients with craniopharyngiomas: a single-center study.J Neurosurg Pediatr. 2018 Jun;21(6):549-562. doi: 10.3171/2017.10.PEDS17254. Epub 2018 Mar 30. J Neurosurg Pediatr. 2018. PMID: 29600905
-
Reoperative endoscopic endonasal surgery for residual or recurrent pituitary adenomas.J Neurosurg. 2017 Aug;127(2):397-408. doi: 10.3171/2016.8.JNS152709. Epub 2016 Oct 28. J Neurosurg. 2017. PMID: 27791524
-
Endoscopic endonasal transsphenoidal approach for pediatric craniopharyngiomas: A case series.Int J Pediatr Otorhinolaryngol. 2020 Mar;130:109786. doi: 10.1016/j.ijporl.2019.109786. Epub 2019 Nov 19. Int J Pediatr Otorhinolaryngol. 2020. PMID: 31812002
-
Endoscopic Endonasal Approach to Giant Pituitary Adenomas: Surgical Outcomes and Review of the Literature.World Neurosurg. 2021 May;149:e1043-e1055. doi: 10.1016/j.wneu.2021.01.019. Epub 2021 Jan 29. World Neurosurg. 2021. PMID: 33524611 Review.
Cited by
-
Giant skull base periosteal chondroma treated with endonasal endoscopic surgery: illustrative case.J Neurosurg Case Lessons. 2024 Jan 22;7(4):CASE23668. doi: 10.3171/CASE23668. Print 2024 Jan 22. J Neurosurg Case Lessons. 2024. PMID: 38252934 Free PMC article.
-
Giant Intracranial Chondroma.Plast Reconstr Surg Glob Open. 2025 May 20;13(5):e6726. doi: 10.1097/GOX.0000000000006726. eCollection 2025 May. Plast Reconstr Surg Glob Open. 2025. PMID: 40395660 Free PMC article.
-
Intracranial extra-axial chondromas: clues to computed tomography and magnetic resonance imaging diagnosis.Acta Neurol Belg. 2024 Oct;124(5):1581-1589. doi: 10.1007/s13760-024-02559-0. Epub 2024 Apr 20. Acta Neurol Belg. 2024. PMID: 38642294
-
A multicenter retrospective analysis of clinical outcomes of intracranial chondrosarcoma in 26 patients.Sci Rep. 2023 Sep 5;13(1):14647. doi: 10.1038/s41598-023-41378-w. Sci Rep. 2023. PMID: 37669996 Free PMC article.
-
Preoperative peripheral inflammatory markers are predictors of postoperative central diabetes insipidus in craniopharyngioma patients: a retrospective study.BMC Cancer. 2024 May 8;24(1):572. doi: 10.1186/s12885-024-12324-4. BMC Cancer. 2024. PMID: 38720306 Free PMC article.
References
LinkOut - more resources
Full Text Sources