

Efficacy and safety of endoscopic duodenal stent versus endoscopic or surgical gastrojejunostomy to treat malignant gastric outlet obstruction: systematic review and meta-analysis
- PMID: 35692924
- PMCID: PMC9187371
- DOI: 10.1055/a-1794-0635
Efficacy and safety of endoscopic duodenal stent versus endoscopic or surgical gastrojejunostomy to treat malignant gastric outlet obstruction: systematic review and meta-analysis
Abstract
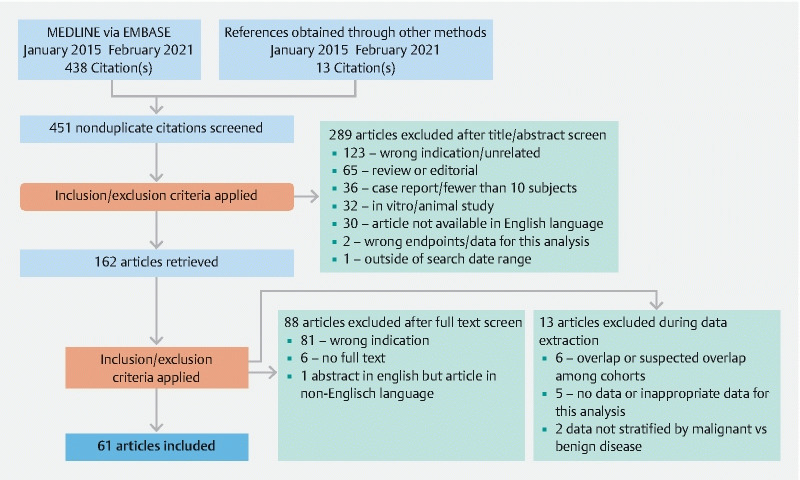
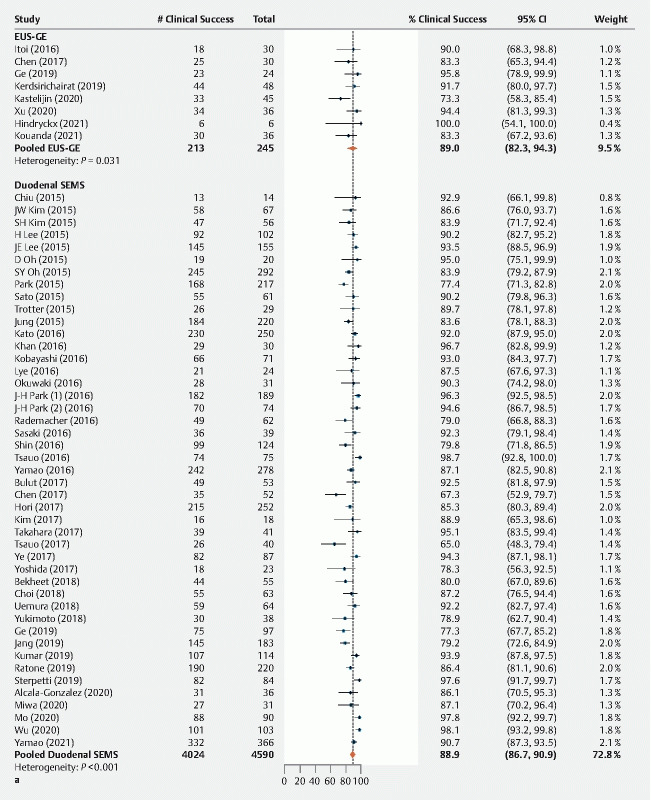
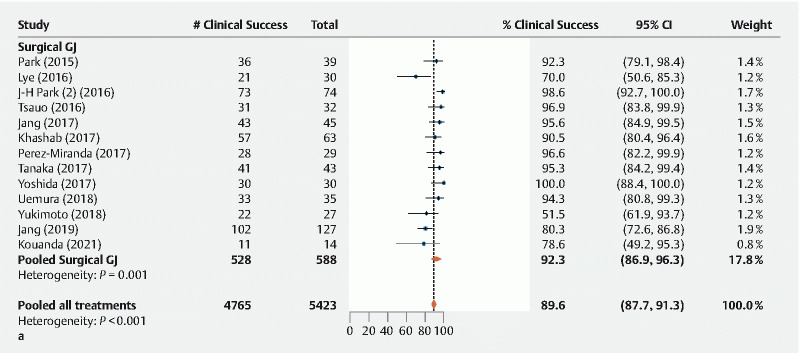
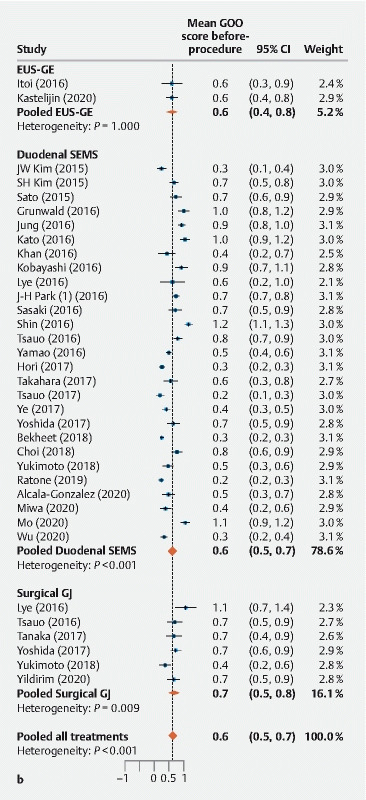
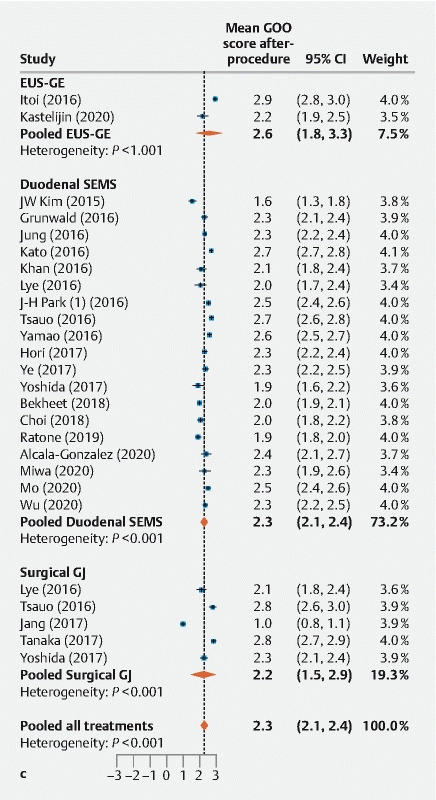
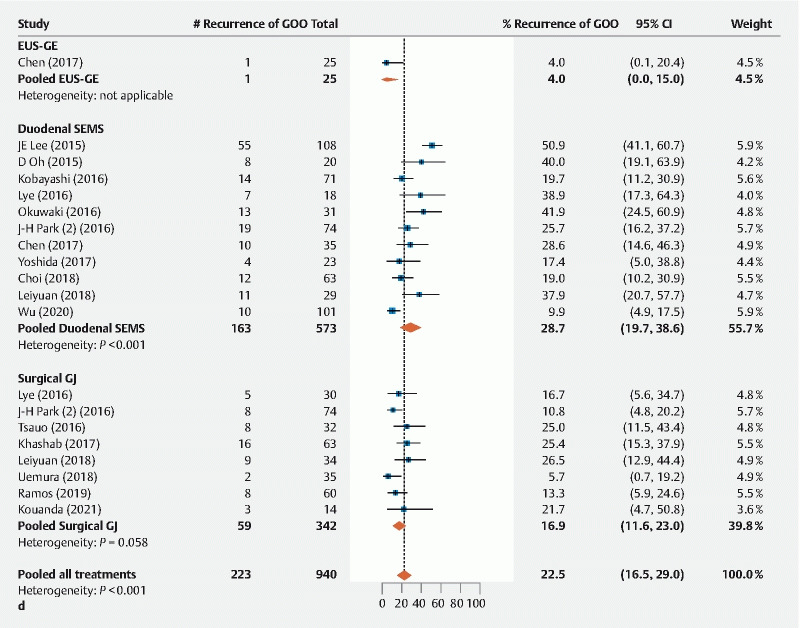
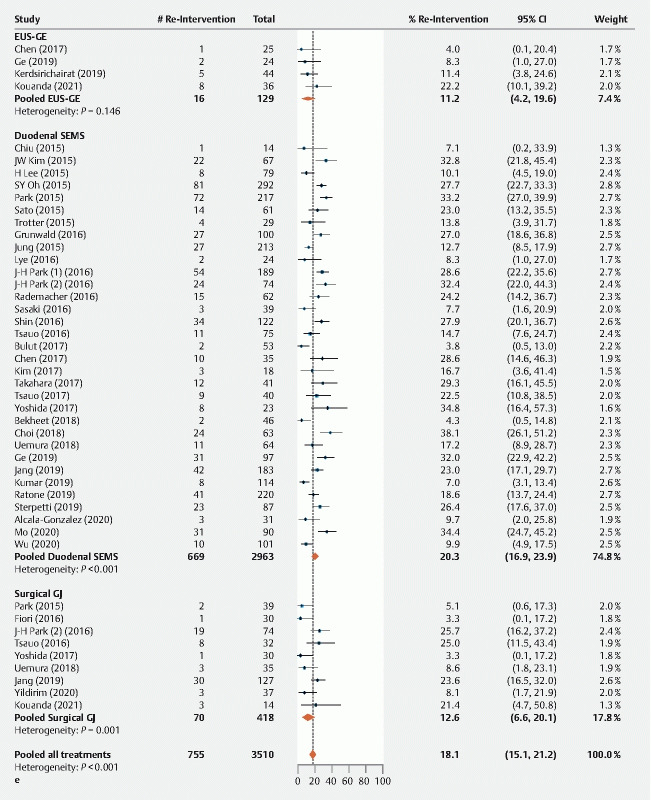
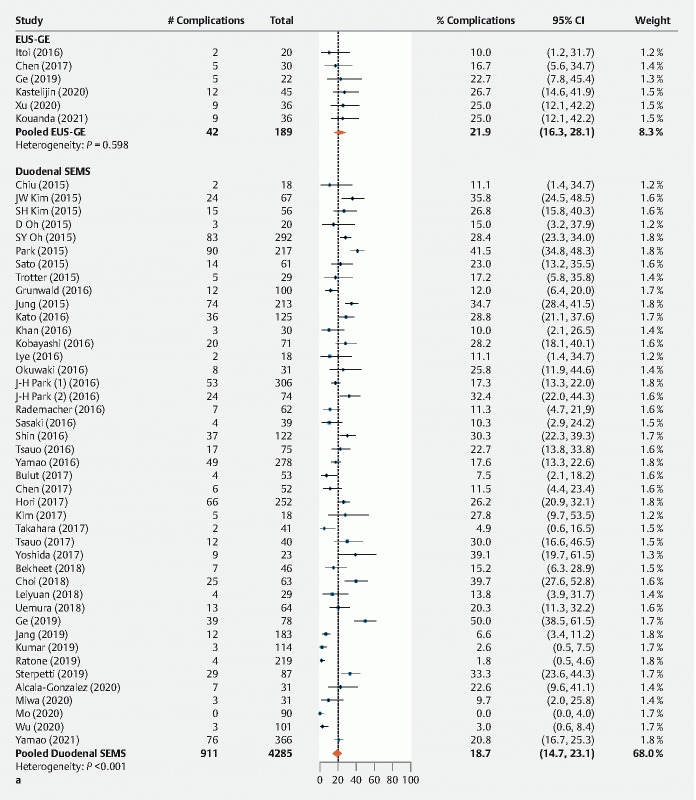
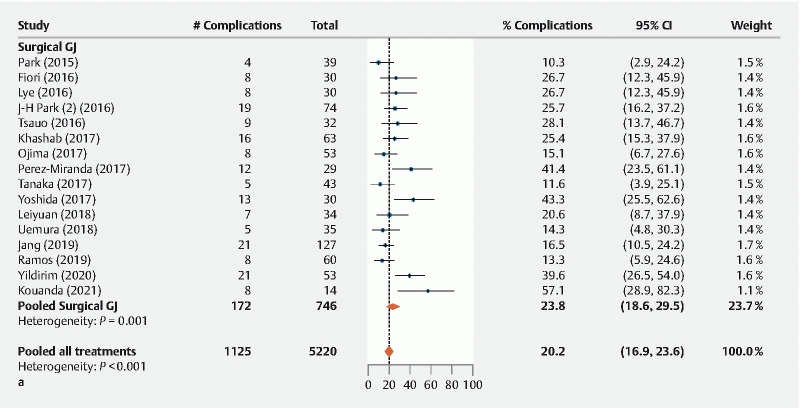
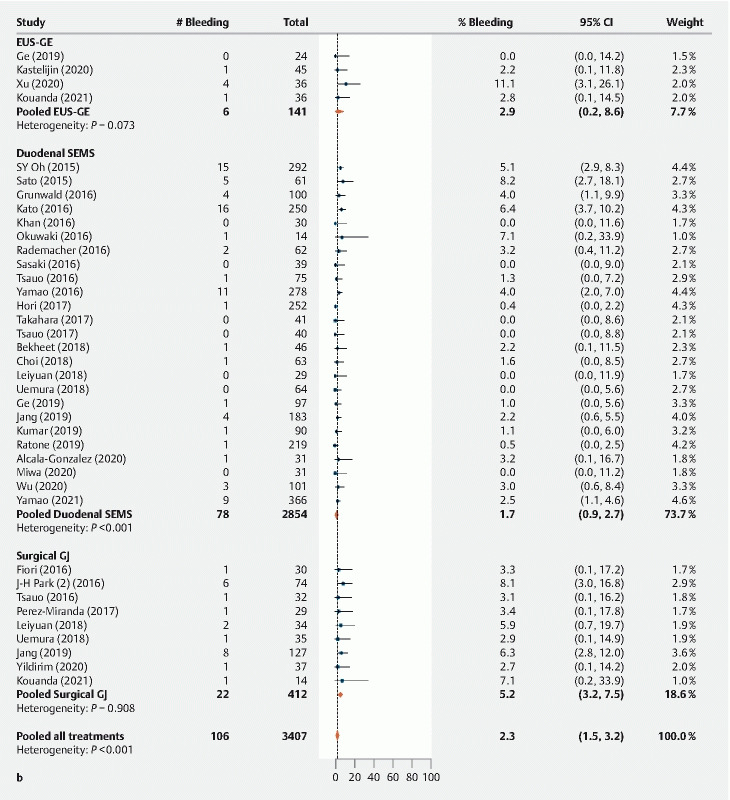
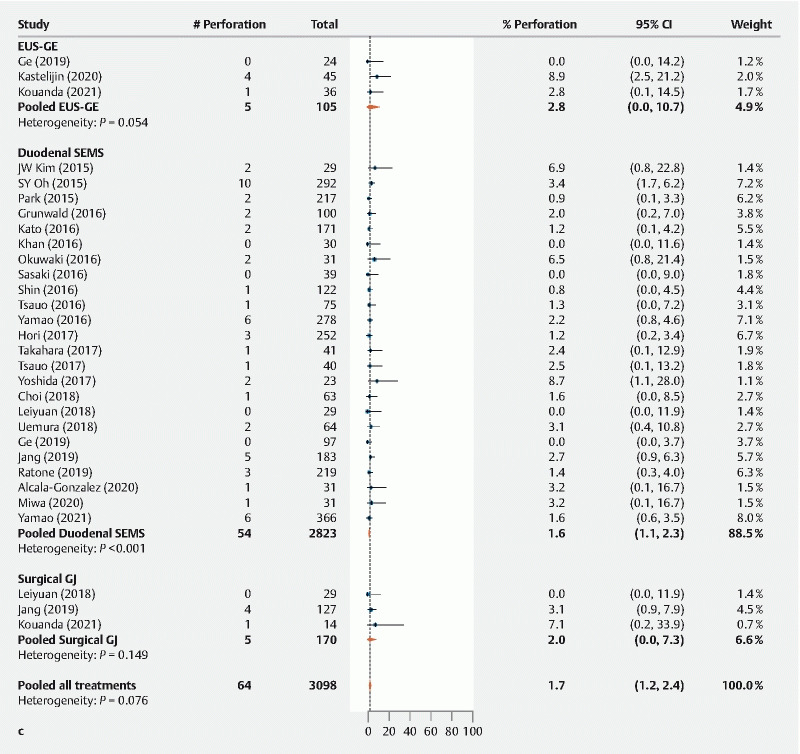
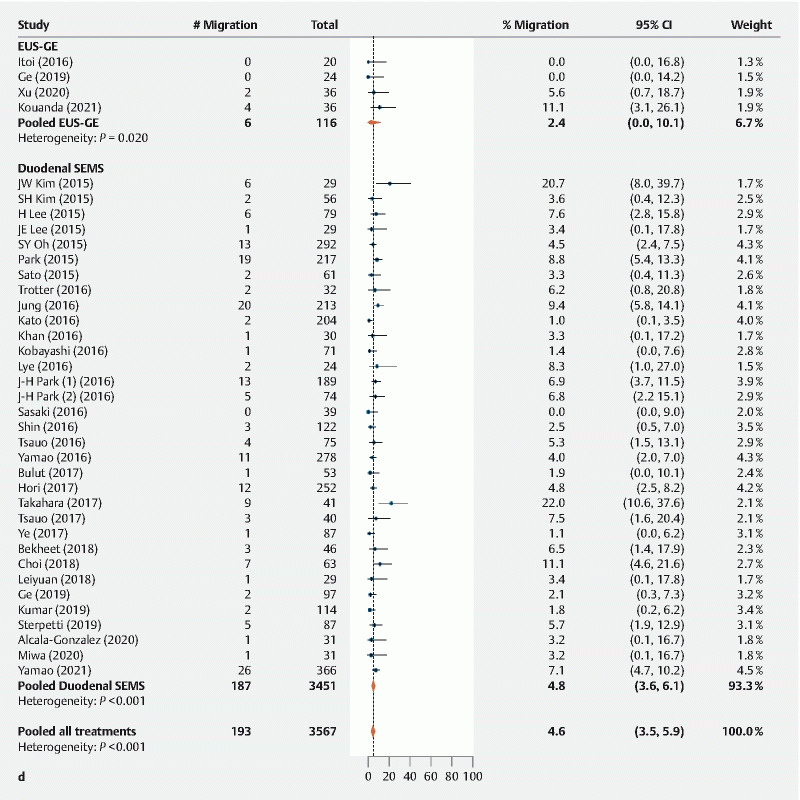
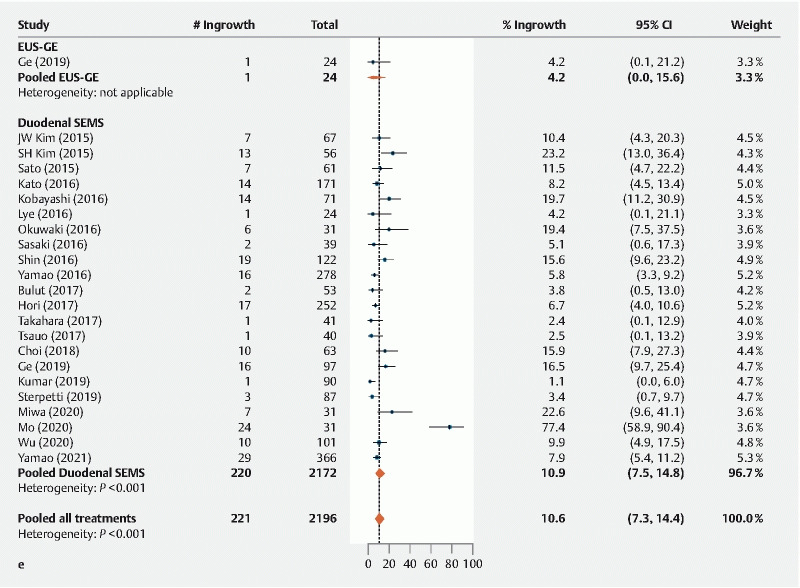
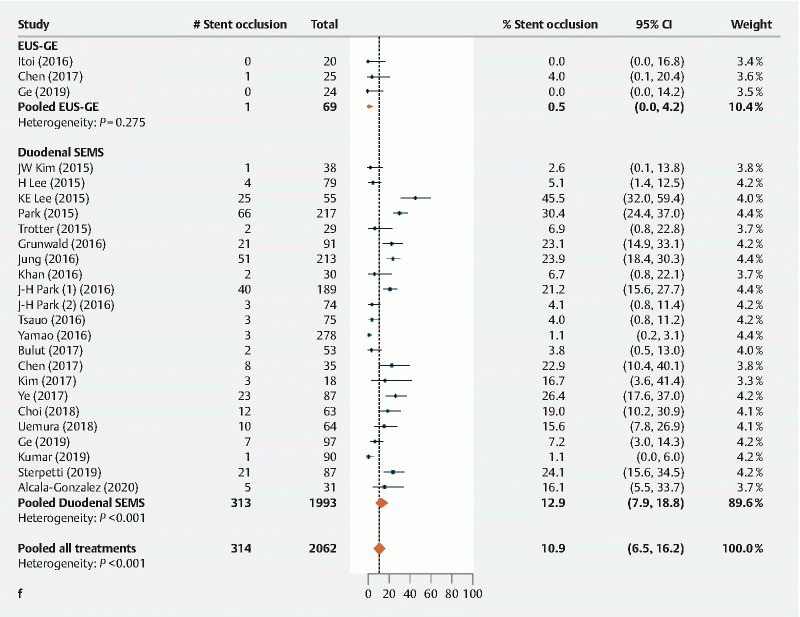
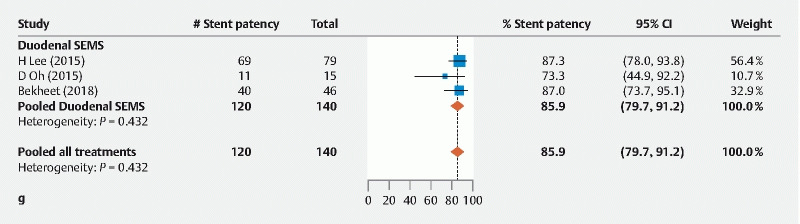
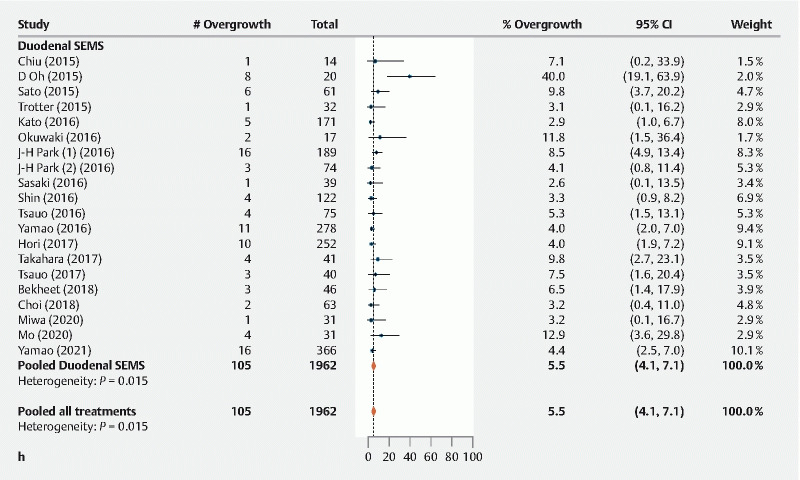
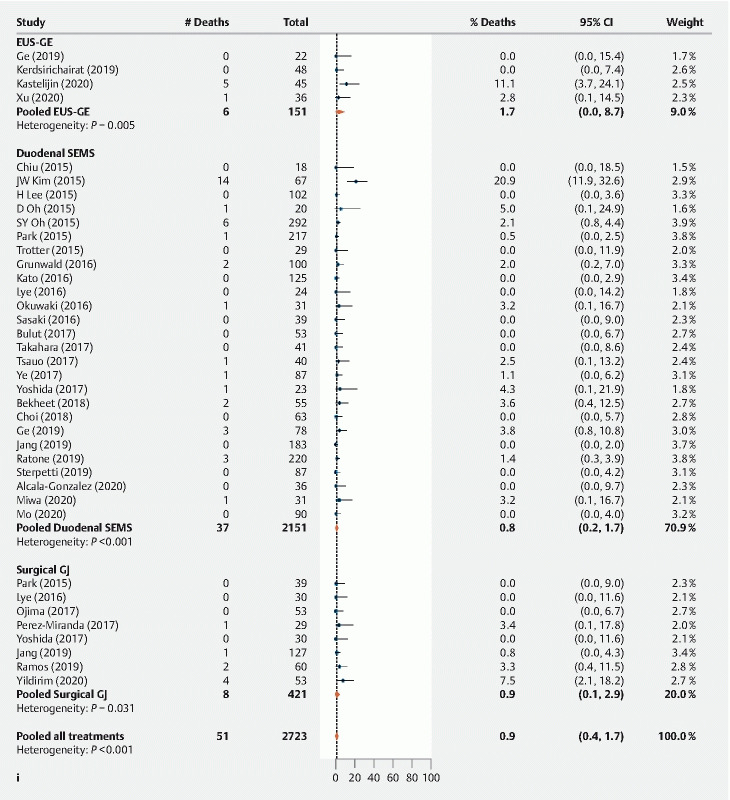
Background and study aims Malignant disease accounts for up to 80 % of gastric outlet obstruction (GOO) cases, which may be treated with duodenal self-expanding metal stents (SEMS), surgical gastrojejunostomy (GJ), and more recently endoscopic-ultrasound-guided gastroenterostomy (EUS-GE). These three treatments have not been compared head-to-head in a randomized trial. Methods We searched the Embase and MEDLINE databases for studies published January 2015-February 2021 assessing treatment of malignant GOO using duodenal SEMS, endoscopic (EUS-GE) or surgical (laparoscopic or open) GJ. Efficacy outcomes assessed included technical and clinical success rates, GOO recurrence and reintervention. Safety outcomes included procedure-related bleeding or perforation, and stent-related events for the duodenal SEMS and EUS-GE arms. Results EUS-GE had a lower rate of technical success (95.3%) than duodenal SEMS (99.4 %) or surgical GJ (99.9%) ( P = 0.0048). For duodenal SEMS vs. EUS-GE vs. surgical GJ, rates of clinical success (88.9 % vs. 89.0 % vs. 92.3 % respectively, P = 0.49) were similar. EUS-GE had a lower rate of GOO recurrence based on limited data ( P = 0.0036), while duodenal SEMS had a higher rate of reintervention ( P = 0.041). Overall procedural complications were similar (duodenal SEMS 18.7 % vs. EUS-GE 21.9 % vs. surgical GJ 23.8 %, P = 0.32), but estimated bleeding rate was lowest ( P = 0.0048) and stent occlusion rate was highest ( P = 0.0002) for duodenal SEMS. Conclusions Duodenal SEMS, EUS-GE, and surgical GJ showed similar clinical efficacy for the treatment of malignant GOO. Duodenal SEMS had a lower procedure-related bleeding rate but higher rate of reintervention.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests Dr. Benias is a consultant for Boston Scientific and Fujifilm. Dr. Kozarek receives research support from Boston Scientific and the National Institutes of Health. Dr. Peetermans, Mr. McMullen and Ms. Gjata are full-time employees of Boston Scientific Corporation. Dr. Irani is a consultant for Boston Scientific and Gore.
Figures
References
-
- Mintziras I, Miligkos M, Wachter S et al.Palliative surgical bypass is superior to palliative endoscopic stenting in patients with malignant gastric outlet obstruction: systematic review and meta-analysis. Surg Endosc. 2019;33:3153–3164. - PubMed
-
- Barthet M, Binmoeller K F, Vanbiervliet G et al.Natural orifice transluminal endoscopic surgery gastroenterostomy with a biflanged lumen-apposing stent: first clinical experience (with videos) Gastrointest Endosc. 2015;81:215–218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources