

Predicting biochemical recurrence of prostate cancer with artificial intelligence
- PMID: 35693032
- PMCID: PMC9177591
- DOI: 10.1038/s43856-022-00126-3
Predicting biochemical recurrence of prostate cancer with artificial intelligence
Abstract
Background: The first sign of metastatic prostate cancer after radical prostatectomy is rising PSA levels in the blood, termed biochemical recurrence. The prediction of recurrence relies mainly on the morphological assessment of prostate cancer using the Gleason grading system. However, in this system, within-grade morphological patterns and subtle histopathological features are currently omitted, leaving a significant amount of prognostic potential unexplored.
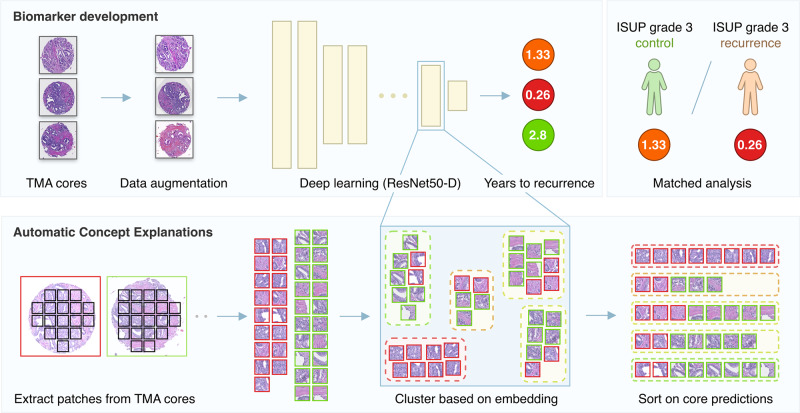
Methods: To discover additional prognostic information using artificial intelligence, we trained a deep learning system to predict biochemical recurrence from tissue in H&E-stained microarray cores directly. We developed a morphological biomarker using convolutional neural networks leveraging a nested case-control study of 685 patients and validated on an independent cohort of 204 patients. We use concept-based explainability methods to interpret the learned tissue patterns.
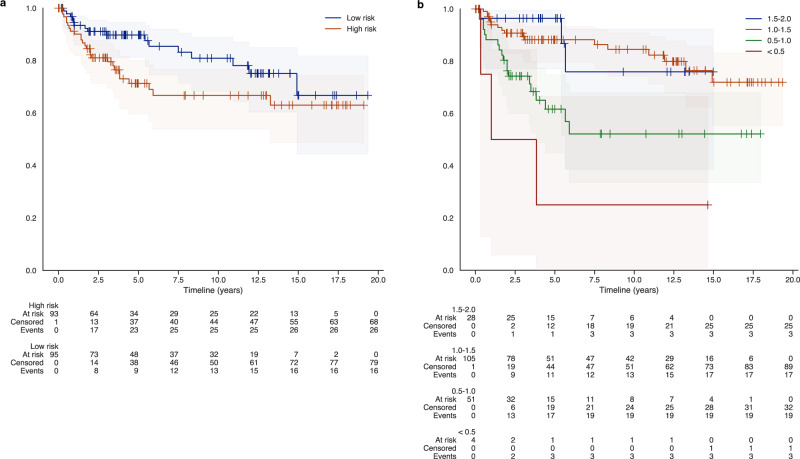
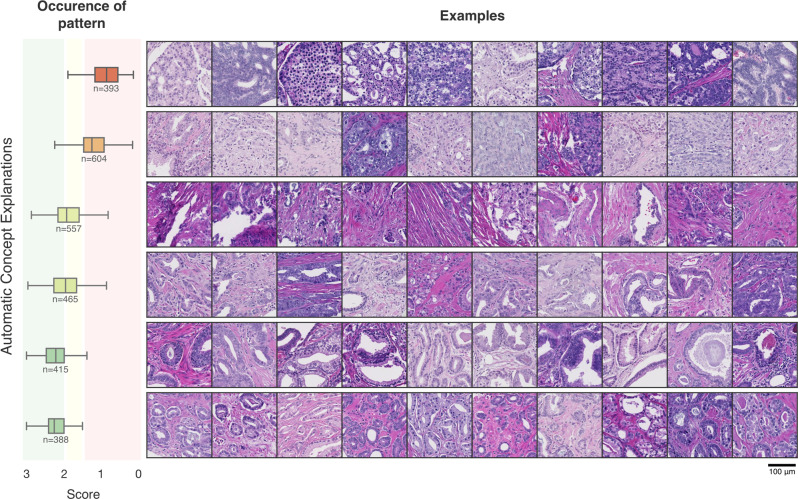
Results: The biomarker provides a strong correlation with biochemical recurrence in two sets (n = 182 and n = 204) from separate institutions. Concept-based explanations provided tissue patterns interpretable by pathologists.
Conclusions: These results show that the model finds predictive power in the tissue beyond the morphological ISUP grading.
Keywords: Epidemiology; Prognostic markers; Prostate; Prostate cancer.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsB.v.G. receive funding and royalties from MeVis Medical Solutions AG, (Bremen, Germany), and reports grants and stock/royalties from Thirona, and grants and royalties from Delft Imaging Systems, all outside the submitted work. J.v.d.L. is a member of the advisory boards of Philips, the Netherlands, and ContextVision, Sweden; and received research funding from Philips, the Netherlands; ContextVision, Sweden; and Sectra, Sweden, all outside the submitted work. G.L. reports research grants from the Dutch Cancer Society, the Netherlands Organization for Scientific Research (NWO), and HealthHolland during the conduct of the study, and grants from Philips Digital Pathology Solutions, and consultancy fees from Novartis and Vital Imaging, outside the submitted work. J.M. is supported by Department of Defense Prostate Cancer Research Program, DOD Award No W81XWH-18-2-0016, PCRP Prostate Cancer Biorepository Network A.D.M. is a paid consultant to Cepheid LLC, and Merck & Co., A.D.M has also received research support from Myriad Genetics and Janssen R&D for other studies. All other authors have no competing interests.
Figures
References
-
- Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.10.3322/caac.21660 (2021). - PubMed
-
- Goonewardene SS, Phull JS, Bahl A, Persad RA. Interpretation of PSA levels after radical therapy for prostate cancer. Trends Urol. Men S Health. 2014;5:30–34. doi: 10.1002/tre.407. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
