

De Novo Glioblastoma Masqueraded within a Hemispheric Dural Meningiomatosis: Rare Imaging Findings and Rationale for Two-Staged Resection
- PMID: 35693250
- PMCID: PMC9179231
- DOI: 10.1055/s-0042-1749215
De Novo Glioblastoma Masqueraded within a Hemispheric Dural Meningiomatosis: Rare Imaging Findings and Rationale for Two-Staged Resection
Abstract
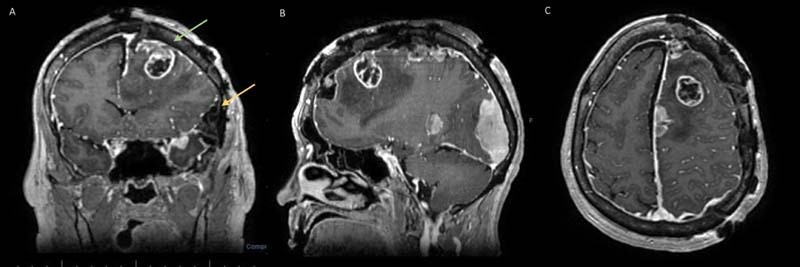
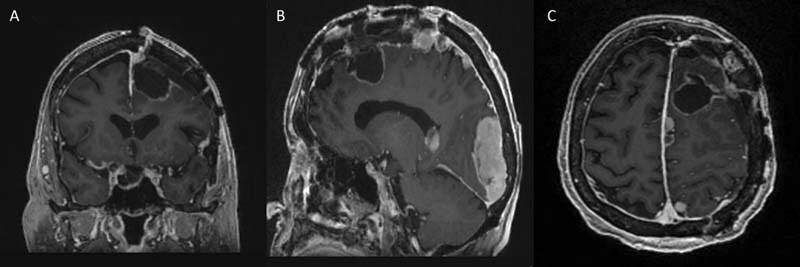
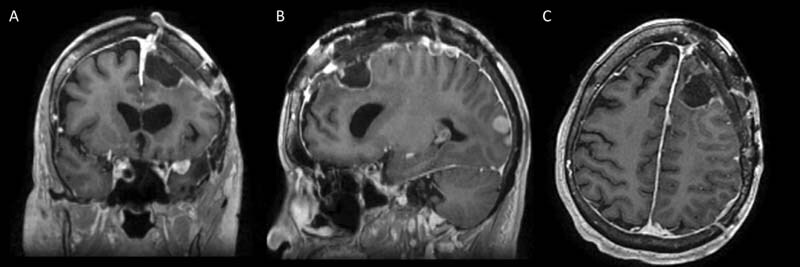
Introduction Collision tumors present as histologically different juxtaposed neoplasms within the same anatomical region, independent of the adjacent cell population. De novo intracranial collision tumors involving metachronous primary brain neoplasms alongside dural meningiomatosis are not well documented in the literature. Clinical Presentation We present staged surgical management of a 72-year-old female with known left hemispheric stable dural-based convexity mass lesions over 10 years and new-onset expressive aphasia and headaches. MRI had revealed left supratentorial dural-based enhanced masses consistent with en plaque meningiomatosis. Embolization angiography showed an unusual tumor blush from an aberrant branch of anterior cerebral artery suggesting a deeper focal intra-axial nature; a stage 1 craniotomy for dural-based tumor resection was completed with diagnosis of a meningioma (WHO grade 1). Intraoperatively, a distinct intra-axial deep discrete lesion was verified stereotactically, concordant with the location of tumor blush. The patient made a complete neurological recovery from a transient postoperative supplemental motor area syndrome in a week. Subsequent postoperative follow-up showed worsening of right hemiparesis and MRI showed an increase in residual lesion size and perilesional edema, which prompted a stage 2 radical resection of a glioblastoma, WHO grade 4. She improved neurologically after surgery with steroids and physical therapy. At 15 months following adjuvant therapy, she remains neurologically intact throughout the postoperative course, with no recurrent tumor on MRI. Conclusion A de novo glioblastoma presented as a masquerading lesion within hemispheric convexity meningiomatosis in an elderly patient with no prior radiation/phakomatosis, inciting a non-causal juxtapositional coexistence. The authors highlight rare pathognomonic angiographic findings and the rationale for two-staged resections of these collision lesions that led to excellent clinicoradiological outcome.
Keywords: case report; collision tumors; glioblastoma; glioma; meningioma; meningiomatosis; supplementary motor area syndrome.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures



References
-
- Sung C T, Shetty A, Menias C O. Collision and composite tumors; radiologic and pathologic correlation. Abdom Radiol (NY) 2017;42(12):2909–2926. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials