

Bone metastases in non-small cell lung cancer: a narrative review
- PMID: 35693589
- PMCID: PMC9186248
- DOI: 10.21037/jtd-21-1502
Bone metastases in non-small cell lung cancer: a narrative review
Abstract
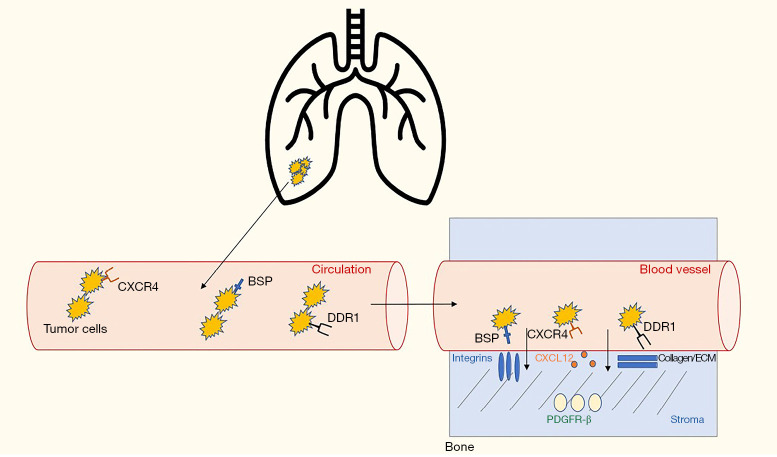
Background and objective: Bone metastases are common in patients with non-small cell lung cancer (NSCLC) and remain a significant source of morbidity, mortality, and diminished quality of life, despite the considerable progress made in the overall management of patients with metastatic NSCLC over the last decade. Understanding the molecular pathogenesis of bone metastases is critical to improving survival, preserving function, and managing symptoms in this patient population. The objective of our review is to provide a comprehensive review of the pathophysiology, clinical presentation, management, and factors predicting the development and prognosis of patients with NSCLC with bone metastases.
Methods: An online electronic search was performed on PubMed and Google Scholar of all English-language literature using combinations of the following keywords: bone metastases, non-small cell lung cancer, pathophysiology, skeletal related events, response to therapy, predictive factors, and immunotherapy. Bibliographies of identified papers were reviewed for additional articles of interest. Observational cohort, retrospective studies, randomized controlled trials (RCTs), meta-analyses, and review articles were examined for this review.
Key content and findings: Bone metastases in lung cancer patients remain a common occurrence, impacting morbidity, mortality, and quality of life. Patients with skeletal related events (SREs) have worse prognosis. There is data supporting use of bisphosphonates and/or denosumab, and these should be considered in all patients with bone metastases. Novel studies comparing the genomic alterations of skeletal metastases and primary tumors are needed. As therapy for patients with advanced disease evolves, more studies are needed to evaluate the interplay between immunotherapy and bone metastases, and in determining the response to treatment in bone.
Conclusions: Predicting development and progression of bone metastases could allow earlier and targeted therapy in patients with bone metastases. Predicting and evaluating response to conventional chemotherapy and immune checkpoint inhibitors in NSCLC patients with bone metastases remains an unmet need and merits further study.
Keywords: Bone metastases; non-small cell lung cancer (NSCLC); skeletal related events (SREs); treatment response.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-21-1502/coif). The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials