

Study design for a multicenter, randomized controlled trial evaluating the diagnostic value of ultrathin bronchoscope compared to thin bronchoscope without fluoroscopy for peripheral pulmonary lesions
- PMID: 35693609
- PMCID: PMC9186243
- DOI: 10.21037/jtd-22-20
Study design for a multicenter, randomized controlled trial evaluating the diagnostic value of ultrathin bronchoscope compared to thin bronchoscope without fluoroscopy for peripheral pulmonary lesions
Abstract
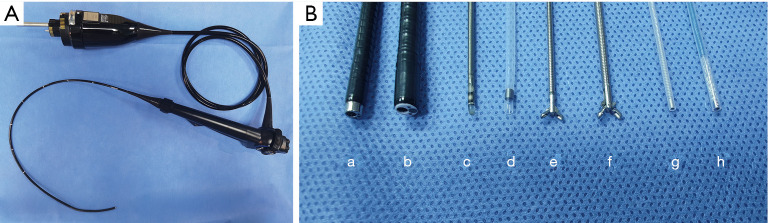
Background: Ultrathin bronchoscope (UTB) with a 3.0-mm outer diameter and a 1.7-mm working channel currently appeared as a potential tool for better biopsy and diagnosis of peripheral pulmonary lesions (PPLs) by accessing more distal bronchus. However, published research is primarily limited to diagnosis value of UTB for PPLs with fluoroscopy, the value of UTB compared with thin bronchoscope (TB) without fluoroscopy guidance has not been determined yet.
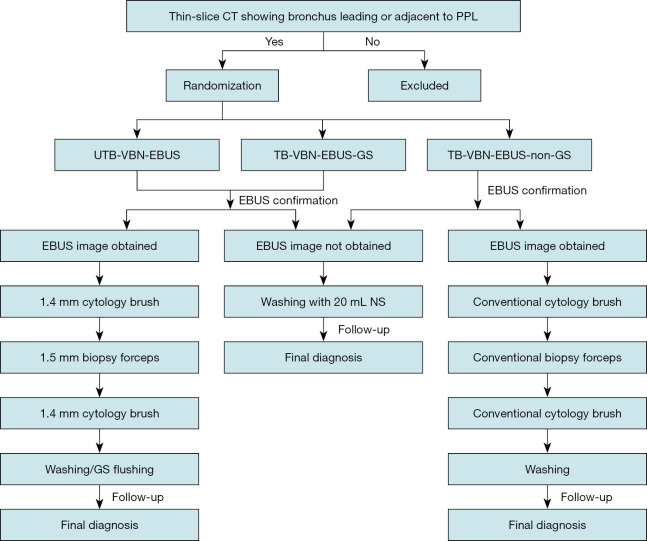
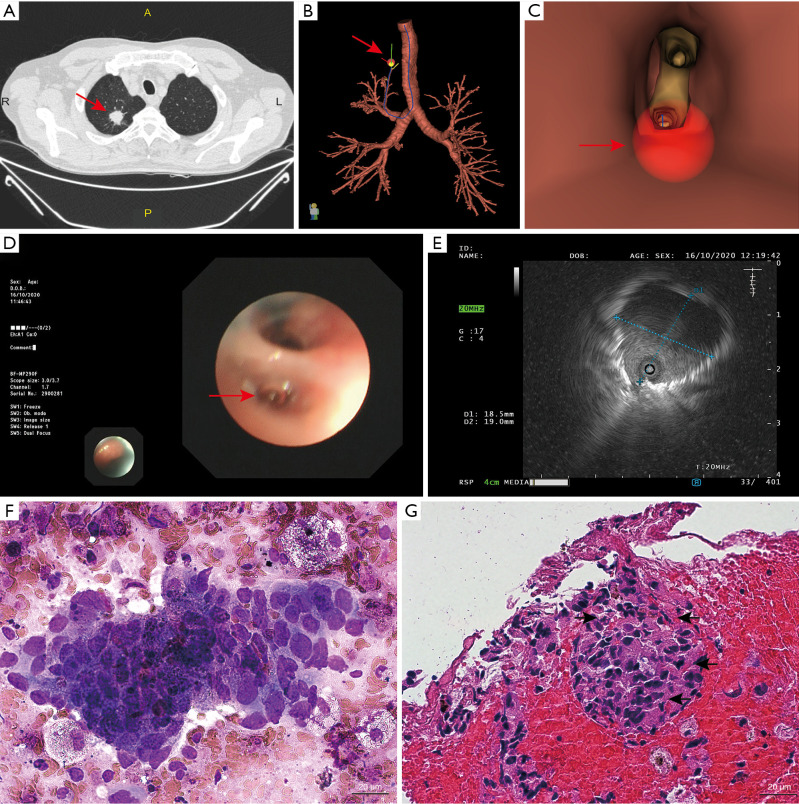
Methods: We design a prospective, randomized, controlled, non-inferior, multicenter study aiming to evaluate the diagnostic value and safety of UTB for PPLs with the guidance of virtual bronchoscopic navigation (VBN) combined with endobronchial ultrasound (EBUS) without fluoroscopy by comparing to TB. The study aims to enroll 578 patients presenting for evaluation of PPLs at five clinical sites in China. Subjects will be randomized to UTB-VBN-EBUS group, TB-VBN-EBUS-guide sheath (GS) group, and TB-VBN-EBUS-non-GS group. Primary endpoint is the diagnostic yield of PPLs. The total examination time, duration of finding lesions, the proportion of lesions visible by radial EBUS, factors affecting the diagnostic yield, difference in the bronchus level reached with the bronchoscope, difference in diagnostic yield, and complication rate will be determined as secondary endpoints. The primary endpoint will be followed-up at least 6-month post-procedure and 1-month post-procedure for safety endpoint.
Discussion: Study enrollment began in March 2021. Our preliminary experience reveals that UTB is a powerful tool in the diagnosis of PPLs even without fluoroscopy. The results of the current study will compensate the limitations of the previous research, further provide evidence of UTB in diagnosing PPLs without fluoroscopy.
Trial registration: ClinicalTrials.gov NCT04571476. Registered on 30 September 2020.
Keywords: Ultrathin bronchoscope (UTB); endobronchial ultrasound (EBUS); peripheral pulmonary lesions (PPLs); thin bronchoscope (TB); virtual bronchoscopic navigation (VBN).
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-20/coif). All authors report funding from Olympus (Beijing) sales and service Co., Ltd.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Medical