

Study Design: Human Leukocyte Antigen Class I Molecule A∗02-Chimeric Antigen Receptor Regulatory T Cells in Renal Transplantation
- PMID: 35694562
- PMCID: PMC9174048
- DOI: 10.1016/j.ekir.2022.03.030
Study Design: Human Leukocyte Antigen Class I Molecule A∗02-Chimeric Antigen Receptor Regulatory T Cells in Renal Transplantation
Abstract
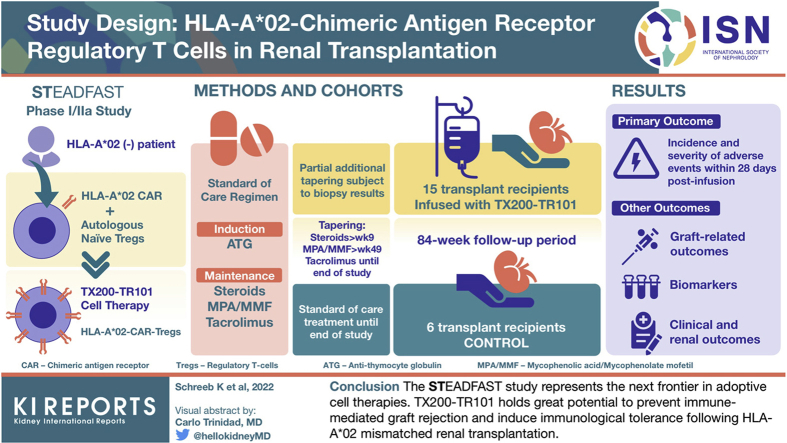
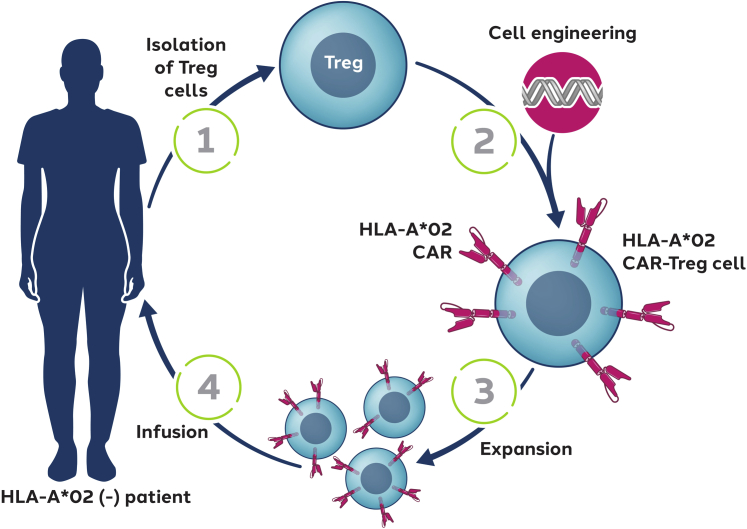
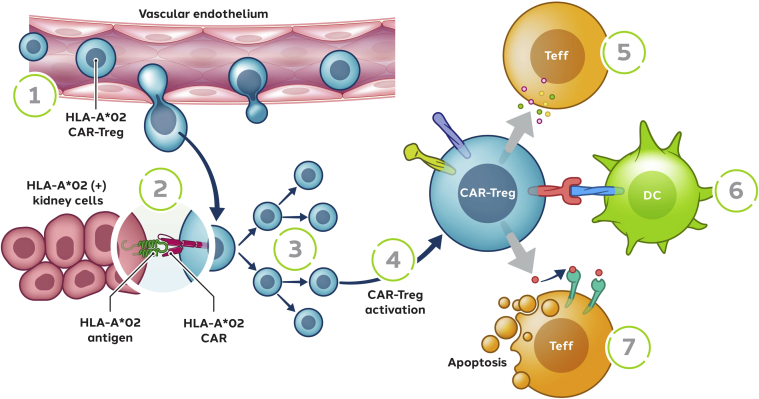
Introduction: Cell therapy with regulatory T cells (Tregs) in solid organ transplantation is a promising approach for the prevention of graft rejection and induction of immunologic tolerance. Previous clinical studies have demonstrated the safety of Tregs in renal transplant recipients. Antigen-specific Tregs, such as chimeric antigen receptor (CAR)-Tregs, are expected to be more efficacious than polyclonal Tregs in homing to the target antigen. We have developed an autologous cell therapy (TX200-TR101) where a human leukocyte antigen (HLA) class I molecule A∗02 (HLA-A∗02)-CAR is introduced into autologous naive Tregs from a patient with HLA-A∗02-negative end-stage renal disease (ESRD) awaiting an HLA-A∗02-positive donor kidney.
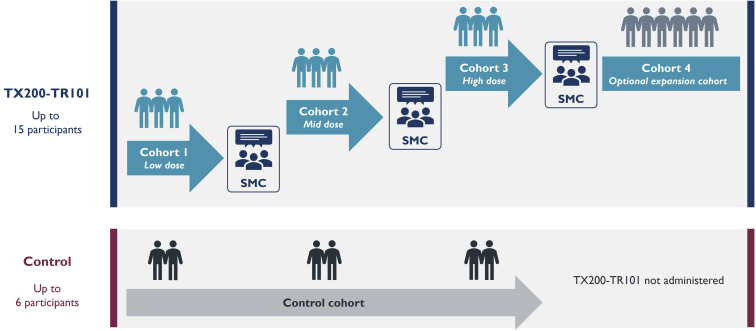
Methods: This article describes the design of the STEADFAST study, a first-in-human, phase I/IIa, multicenter, open-label, single-ascending dose, dose-ranging study to assess TX200-TR101 in living-donor renal transplant recipients. Up to 15 transplant recipients will receive TX200-TR101 and will be followed up for a total of 84 weeks post-transplant, alongside a control cohort of up to 6 transplant recipients. All transplant recipients will receive a standard of care immunosuppressive regimen, with the intent of intensified tapering of the regimen in the TX200-TR101 cohort.
Results: The primary end point is the incidence and severity of treatment-emergent adverse events (AEs) within 28 days post-TX200-TR101 infusion. Other end points include additional safety parameters, clinical and renal outcome parameters, and the evaluation of biomarkers.
Conclusion: The STEADFAST study represents the next frontier in adoptive cell therapies. TX200-TR101 holds great potential to prevent immune-mediated graft rejection and induce immunologic tolerance after HLA-A∗02-mismatched renal transplantation.
Keywords: CAR-Tregs; HLA-A∗02 mismatch; acute and chronic kidney rejection; end-stage renal disease; immunotherapy; living-donor kidney transplantation.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
