

Assessing Concurrent Adherence to Combined Essential Medication and Clinical Outcomes in Patients With Acute Coronary Syndrome. A Population-Based, Real-World Study Using Group-Based Trajectory Models
- PMID: 35694663
- PMCID: PMC9174582
- DOI: 10.3389/fcvm.2022.863876
Assessing Concurrent Adherence to Combined Essential Medication and Clinical Outcomes in Patients With Acute Coronary Syndrome. A Population-Based, Real-World Study Using Group-Based Trajectory Models
Abstract
Aim: Adherence to multiple medications recommended for secondary prevention of cardiovascular conditions represents a challenge. We aimed to identify patterns of concurrent adherence to combined therapy and assess their impact on clinical outcomes in a cohort of patients with acute coronary syndrome (ACS).
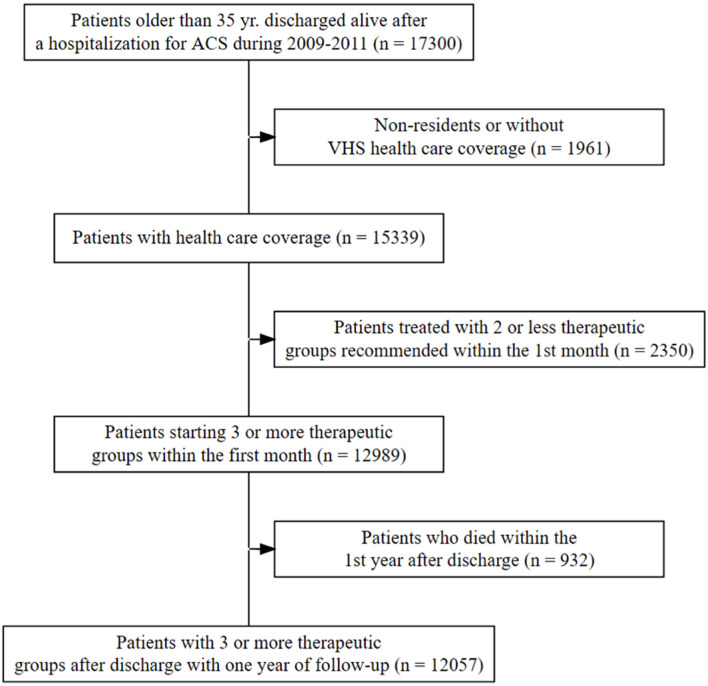
Methods: Population-based retrospective cohort of all patients discharged after hospitalization for ACS (2009-2011), prescribed ≥3 therapeutic groups within the first month. We assessed monthly concurrent adherence (≥24 days of medication out of 30) to ≥3 medications during the first year, and patterns were identified through group-based trajectory models. A composite clinical outcome during the second year was constructed. The association between adherence patterns and traditional refill adherence metrics [e.g., the proportion of days covered (PDC)], and outcomes were assessed through a multivariable Cox proportional hazards model.
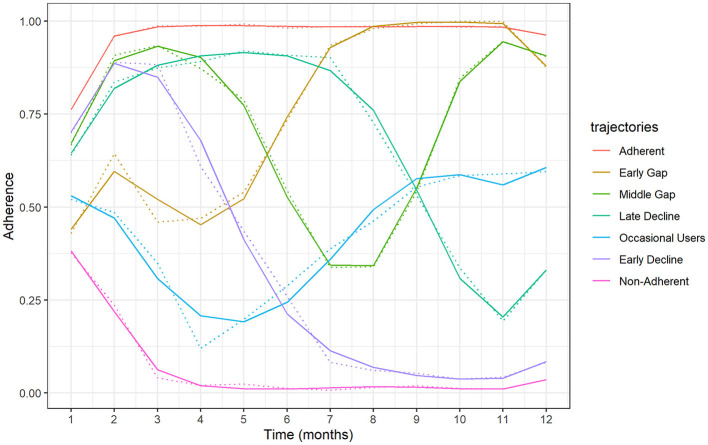
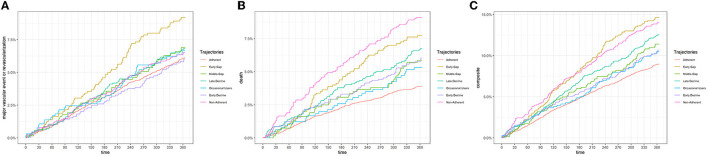
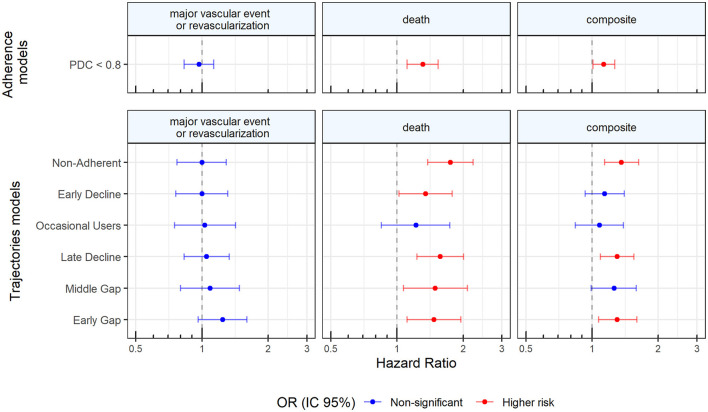
Results: Among 15,797 patients discharged alive, 12,057 (76.32%) initiated treatment with ≥3 therapeutic groups after discharge. We identified seven adherence trajectories to ≥3 medications: Adherent (52.94% of patients); Early Gap (6.64%); Middle Gap (5.67%); Late Decline (10.93%); Occasional Users (5.45%); Early Decline (8.79%); Non-Adherent (9.58%). Compared to the Adherent group, patients belonging to Early Gap (HR:1.30, 95%CI 1.07;1.60), Late decline (hazards ratio (HR): 1.31, 95% CI 1.1; 1.56), and Non-Adherent trajectories (HR: 1.36, 95% CI 1.14; 1.63) had a greater risk of adverse clinical outcomes, which was also different to the risk ascertained through concurrent PDC < 80 (HR: 1.13, 95% CI 1.01; 1.27).
Conclusion: Overall, seven adherence trajectories to ≥3 drugs were identified, with three distinct adherence patterns being at higher risk of adverse outcomes. The identification of patterns of concurrent adherence, a more comprehensive approach than traditional measurements, may be useful to target interventions to improve adherence to multiple medications.
Keywords: acute coronary syndrome; clinical outcomes; concomitant medications; concurrent adherence; group-based trajectory models; population-based cohort; real-world data.
Copyright © 2022 Rodríguez-Bernal, Sánchez-Saez, Bejarano-Quisoboni, Hurtado, García-Sempere, Peiró and Sanfélix-Gimeno.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. (2013) 127:e362–425. 10.1161/CIR.0b013e3182742c84 - DOI - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. (2014) 130:e344–426. 10.1161/CIR.0000000000000134 - DOI - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. (2013) 34:2949–3003. 10.1093/eurheartj/eht296 - DOI - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2016) 37:267–315. 10.1093/eurheartj/ehv320 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous