

Laparoscopic versus open lateral pelvic lymph node dissection in locally advanced rectal cancer: multicentre retrospective cohort study
- PMID: 35694967
- PMCID: PMC9189607
- DOI: 10.1093/bjsopen/zrac068
Laparoscopic versus open lateral pelvic lymph node dissection in locally advanced rectal cancer: multicentre retrospective cohort study
Abstract
Background: Lateral pelvic lymph node dissection (LPLND) is an option in the treatment of rectal cancer and may reduce local recurrence/improve disease-free survival. Advancements in minimally invasive technology have improved the ability to identify anatomy and neurovascular structures that may help in LPLND. The aim of this retrospective study was to evaluate the technical feasibility and oncological safety of laparoscopic LPLND compared with the open LPLND.
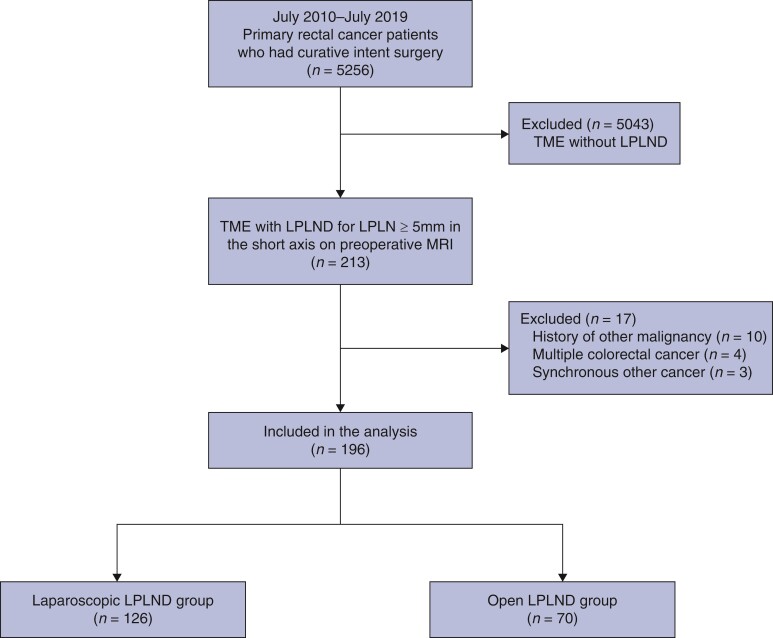
Method: Between July 2010 and July 2019, patients from three tertiary referral hospitals who underwent LPLND with total mesorectal excision for primary rectal cancer were included. Baseline patient characteristics, perioperative outcomes, pathologic results, recurrence, and survival were compared between the laparoscopic and open groups.
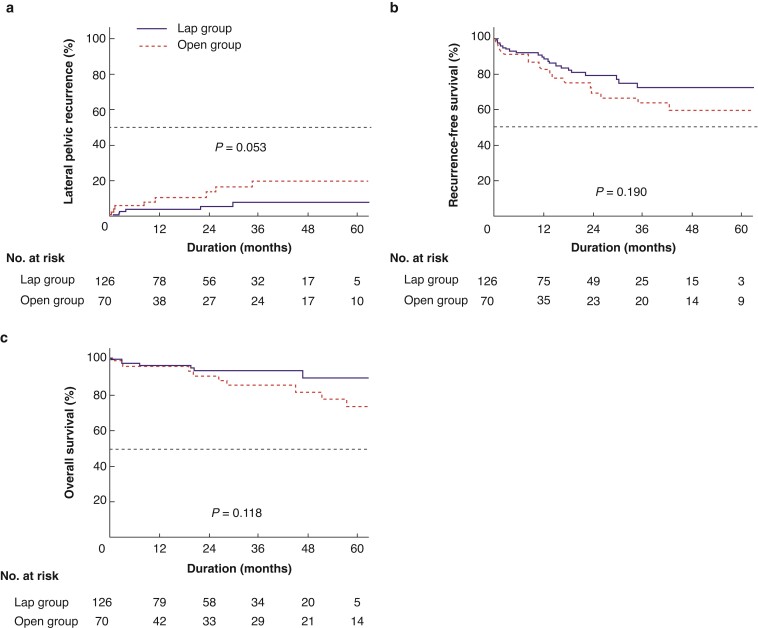
Results: There were 126 and 70 patients in the laparoscopic and open groups respectively. The laparoscopic group had less estimated blood loss (100 ml versus 300 ml, P < 0.001) and lower transfusion rate (0.8 per cent versus 10.0 per cent; P = 0.003) but longer operating times (318 min versus 270 min, P = 0.004). The laparoscopic group had fewer wound infections (1.6 per cent versus 10.0 per cent, P = 0.011) and neuropathy (0 per cent versus 4.3 per cent, P = 0.044). Lateral pelvic recurrence rate was 7.6 per cent in the laparoscopic group and 19.6 per cent in the open group (P = 0.053). Recurrence-free survival (72.2 per cent versus 63.5 per cent; P = 0.190) and overall survival (93.3 per cent versus 85.0 per cent; P = 0.118) were not significantly different.
Conclusion: Laparoscopic LPLND was associated with improved perioperative outcomes and non-inferior oncological outcomes.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Temple WJ, Saettler EB. Locally recurrent rectal cancer: role of composite resection of extensive pelvic tumors with strategies for minimizing risk of recurrence. J Surg Oncol 2000;73:47–58 - PubMed
-
- Garcia-Aguilar J, Cromwell JW, Marra C, Lee SH, Madoff RD, Rothenberger DA. Treatment of locally recurrent rectal cancer. Dis Colon Rectum 2001;44:1743–1748 - PubMed
-
- Heald RJ, Ryall RDH. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;327:1479–1482. - PubMed
-
- Havenga K, Enker WE, Norstein J, Moriya Y, Heald RJ, Van Houwelingen HCet al. Improved survival and local control after total mesorectal excision or D3 lymphadenectomy in the treatment of primary rectal cancer: an international analysis of 1411 patients. Eur J Surg Oncol 1999;25:368–374 - PubMed
-
- Folkesson J, Birgisson H, Pahlman L, Cedermark B, Glimelius B, Gunnarsson U. Swedish rectal cancer trial: long lasting benefits from radiotherapy on survival and local recurrence rate. J Clin Oncol 2005;23:5644–5650 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
