

Using generalized additive models to decompose time series and waveforms, and dissect heart-lung interaction physiology
- PMID: 35695942
- PMCID: PMC9852126
- DOI: 10.1007/s10877-022-00873-7
Using generalized additive models to decompose time series and waveforms, and dissect heart-lung interaction physiology
Abstract
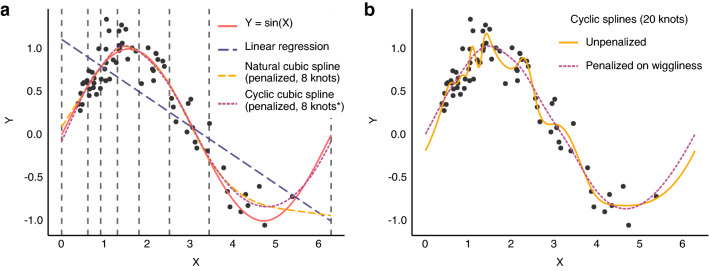
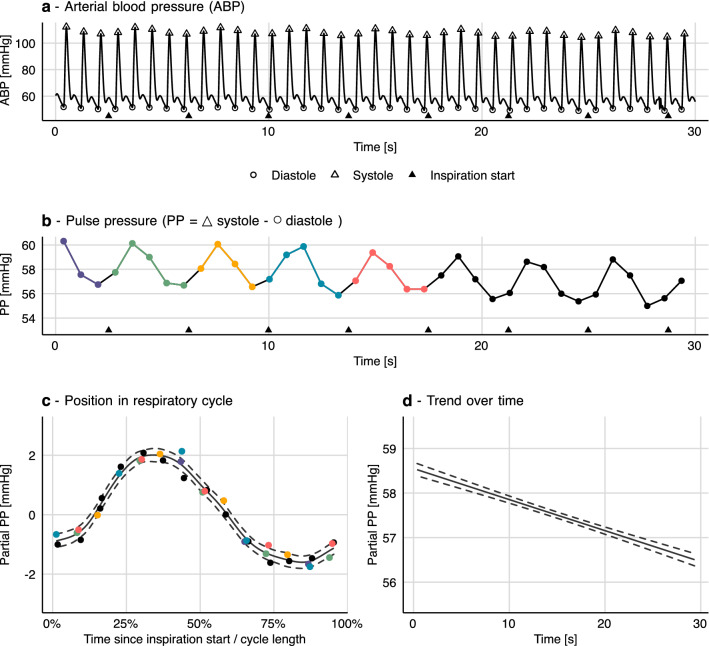
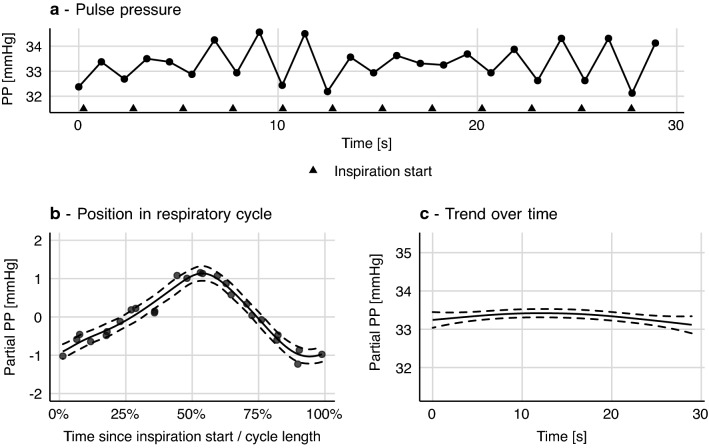
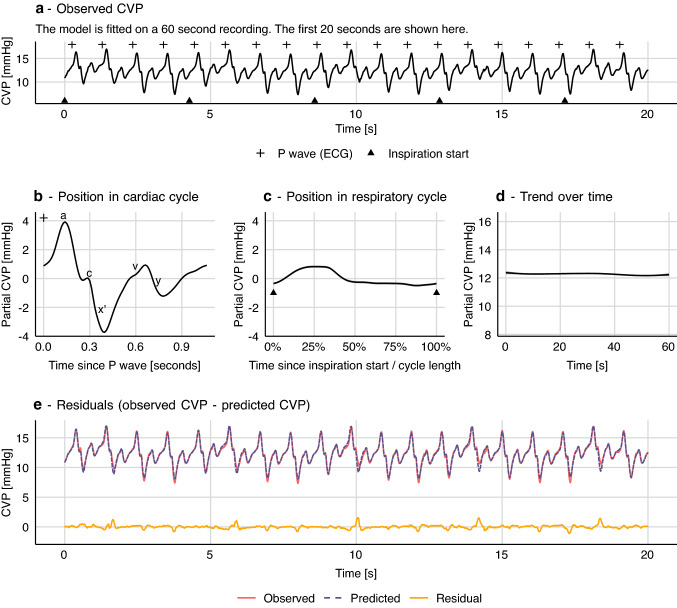
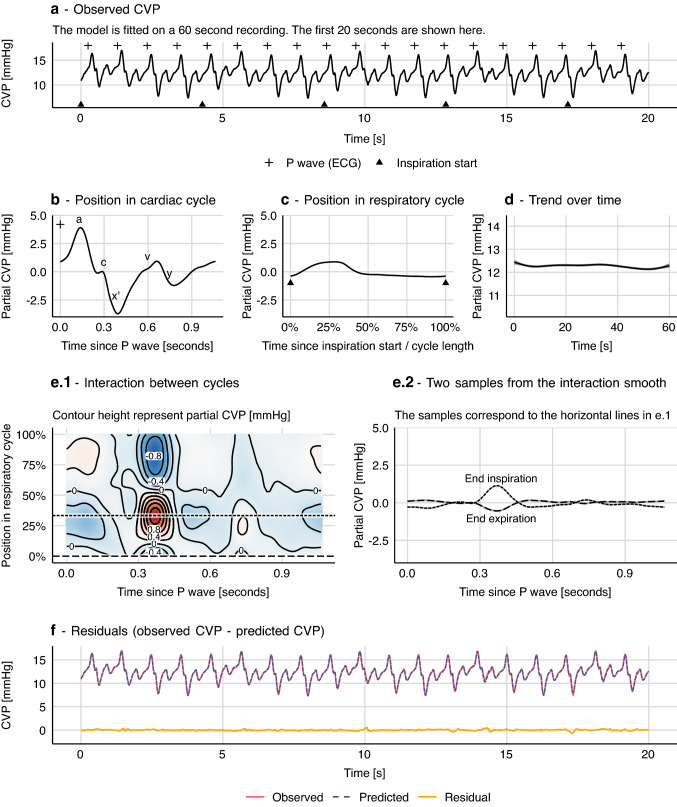
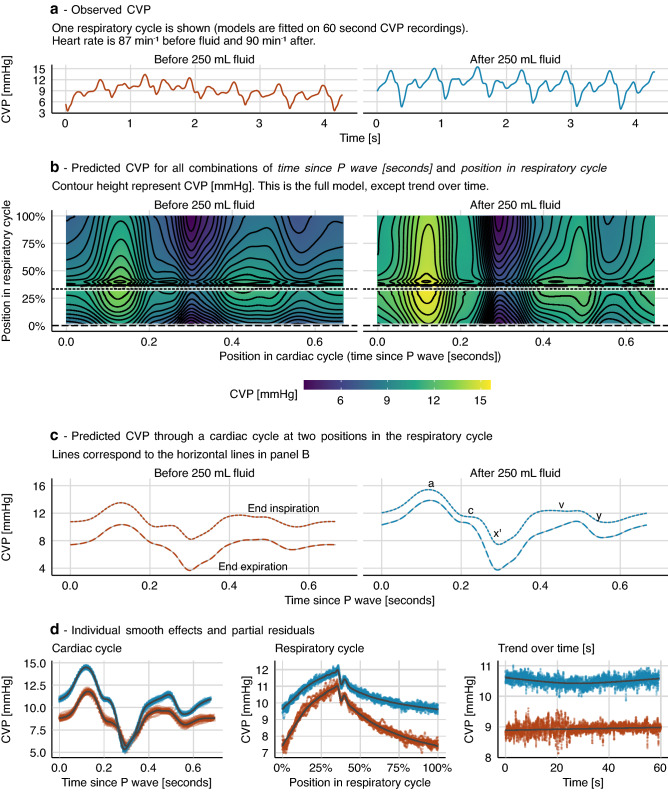
Common physiological time series and waveforms are composed of repeating cardiac and respiratory cycles. Often, the cardiac effect is the primary interest, but for, e.g., fluid responsiveness prediction, the respiratory effect on arterial blood pressure also convey important information. In either case, it is relevant to disentangle the two effects. Generalized additive models (GAMs) allow estimating the effect of predictors as nonlinear, smooth functions. These smooth functions can represent the cardiac and respiratory cycles' effects on a physiological signal. We demonstrate how GAMs allow a decomposition of physiological signals from mechanically ventilated subjects into separate effects of the cardiac and respiratory cycles. Two examples are presented. The first is a model of the respiratory variation in pulse pressure. The second demonstrates how a central venous pressure waveform can be decomposed into a cardiac effect, a respiratory effect and the interaction between the two cycles. Generalized additive models provide an intuitive and flexible approach to modelling the repeating, smooth, patterns common in medical monitoring data.
Keywords: Central venous pressure; Hemodynamic monitoring; Mechanical ventilation; Signal processing; Statistical modelling.
© 2022. The Author(s).
Conflict of interest statement
STV is associate editor of Journal of Clinical Monitoring and Computing. JE and GLS report no competing interests.
Figures

References
-
- Hastie T, Tibshirani R. Generalized additive models. Stat Sci Inst Math Stat. 1986;1:297–318.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
