

Loop diuretics in adult intensive care patients with fluid overload: a systematic review of randomised clinical trials with meta-analysis and trial sequential analysis
- PMID: 35696008
- PMCID: PMC9192894
- DOI: 10.1186/s13613-022-01024-6
Loop diuretics in adult intensive care patients with fluid overload: a systematic review of randomised clinical trials with meta-analysis and trial sequential analysis
Abstract
Background: Fluid overload is a risk factor for organ dysfunction and death in intensive care unit (ICU) patients, but no guidelines exist for its management. We systematically reviewed benefits and harms of a single loop diuretic, the predominant treatment used for fluid overload in these patients.
Methods: We conducted a systematic review with meta-analysis and Trial Sequential Analysis (TSA) of a single loop diuretic vs. other interventions reported in randomised clinical trials, adhering to our published protocol, the Cochrane Handbook, and PRISMA statement. We assessed the risks of bias with the ROB2-tool and certainty of evidence with GRADE. This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42020184799).
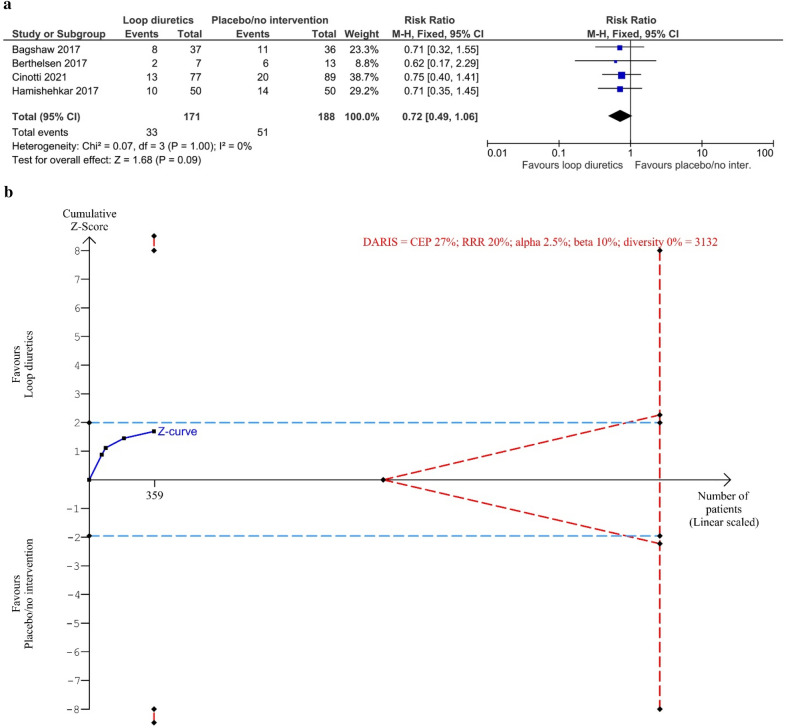
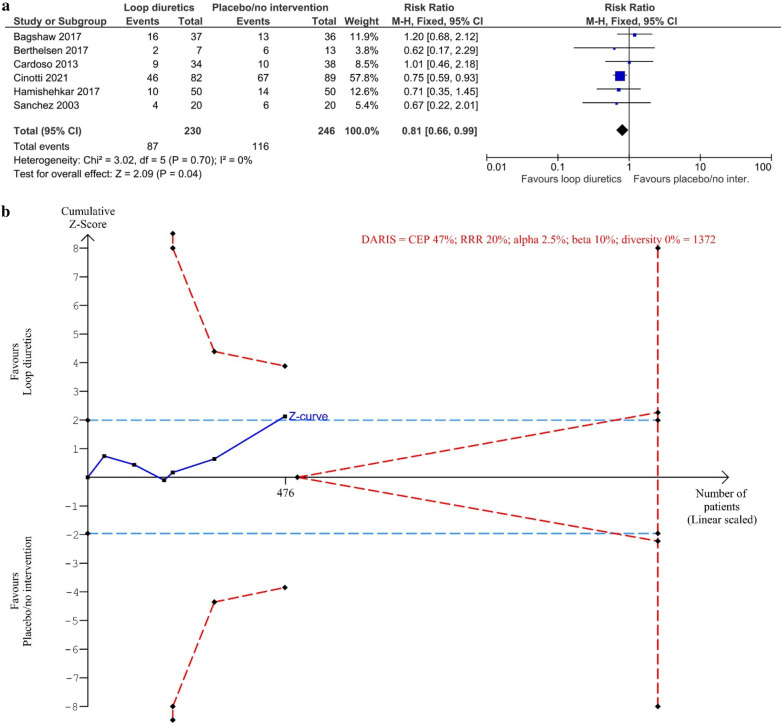
Results: We included 10 trials (804 participants), all at overall high risk of bias. For loop diuretics vs. placebo/no intervention, we found no difference in all-cause mortality (relative risk (RR) 0.72, 95% confidence interval (CI) 0.49-1.06; 4 trials; 359 participants; I2 = 0%; TSA-adjusted CI 0.15-3.48; very low certainty of evidence). Fewer serious adverse events were registered in the group treated with loop diuretics (RR 0.81, 95% CI 0.66-0.99; 6 trials; 476 participants; I2 = 0%; very low certainty of evidence), though contested by TSA (TSA-adjusted CI 0.55-1.20).
Conclusions: The evidence is very uncertain about the effect of loop diuretics on mortality and serious adverse events in adult ICU patients with fluid overload. Loop diuretics may reduce the occurrence of these outcomes, but large randomised placebo-controlled trials at low risk of bias are needed.
Keywords: Critical care; Diuretics; Fluid accumulation; Fluid overload; Furosemide; Loop diuretics; Systematic review.
© 2022. The Author(s).
Conflict of interest statement
SW, TSI, REB and MBH: The Dept. of Intensive Care, Copenhagen University Hospital, North Zealand receives support for research from the Novo Nordisk Foundation, Jacob Madsen’s and wife Olga Madsen’s Foundation, Svend Andersen’s Foundation, Merchant Jakob Ehrenreich and wife Grete Ehrenreich’s Foundation, and Health Insurance Denmark (Sygeforsikringen Danmark). MB, NL, JL and CG: None known. AP: The Dept. of Intensive Care, Rigshospitalet receives support for research from the Novo Nordisk Foundation, Health Insurance Denmark (Sygeforsikringen Danmark), Fresenius Kabi, Denmark, and Pfizer, Denmark.
Figures
Similar articles
-
Loop diuretics in adult intensive care patients with fluid overload: A protocol for a systematic review of randomised clinical trials with meta-analysis and Trial Sequential Analysis.Acta Anaesthesiol Scand. 2020 Oct;64(9):1327-1334. doi: 10.1111/aas.13655. Epub 2020 Jul 15. Acta Anaesthesiol Scand. 2020. PMID: 32531069
-
Goal directed fluid removal with furosemide versus placebo in intensive care patients with fluid overload: A trial protocol for a randomised, blinded trial (GODIF trial).Acta Anaesthesiol Scand. 2022 Oct;66(9):1138-1145. doi: 10.1111/aas.14121. Epub 2022 Aug 9. Acta Anaesthesiol Scand. 2022. PMID: 35898170 Free PMC article.
-
Comparison of all types of loop-diuretics for chronic heart failure: A protocol for a systematic review and network meta-analysis.Acta Anaesthesiol Scand. 2025 Mar;69(3):e70005. doi: 10.1111/aas.70005. Acta Anaesthesiol Scand. 2025. PMID: 39961678
-
N-acetylcysteine for non-paracetamol (acetaminophen)-related acute liver failure.Cochrane Database Syst Rev. 2020 Dec 9;12(12):CD012123. doi: 10.1002/14651858.CD012123.pub2. Cochrane Database Syst Rev. 2020. PMID: 33294991 Free PMC article.
-
Prophylaxis of thromboembolism during therapy with asparaginase in adults with acute lymphoblastic leukaemia.Cochrane Database Syst Rev. 2020 Oct 10;10(10):CD013399. doi: 10.1002/14651858.CD013399.pub2. Cochrane Database Syst Rev. 2020. PMID: 33038027 Free PMC article.
Cited by
-
Fluid accumulation in adult ICU patients - A protocol for a scoping review.Acta Anaesthesiol Scand. 2025 Mar;69(3):e14584. doi: 10.1111/aas.14584. Acta Anaesthesiol Scand. 2025. PMID: 39853691 Free PMC article. Review.
-
Nordic survey on assessment and treatment of fluid overload in intensive care.Front Med (Lausanne). 2022 Nov 25;9:1067162. doi: 10.3389/fmed.2022.1067162. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36507497 Free PMC article.
-
Effect of manual decongestive therapy on cardiac preload in critically ill patients: a randomized controlled trial.Ann Intensive Care. 2025 Mar 24;15(1):39. doi: 10.1186/s13613-025-01453-z. Ann Intensive Care. 2025. PMID: 40126737 Free PMC article.
-
Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup.Nat Rev Nephrol. 2023 Jun;19(6):401-417. doi: 10.1038/s41581-023-00683-3. Epub 2023 Feb 23. Nat Rev Nephrol. 2023. PMID: 36823168 Review.
-
Administration of Intravenous Furosemide in Patients with Acute Infection: Patient Characteristics and Impact on In-Hospital Outcome.J Clin Med. 2023 May 16;12(10):3496. doi: 10.3390/jcm12103496. J Clin Med. 2023. PMID: 37240603 Free PMC article.
References
-
- Van Regenmortel N, Moers L, Langer T, Roelant E, De Weerdt T, Caironi P, et al. Fluid-induced harm in the hospital: look beyond volume and start considering sodium. From physiology towards recommendations for daily practice in hospitalized adults. Ann Intensive Care. 2021;11:79. doi: 10.1186/s13613-021-00851-3. - DOI - PMC - PubMed
-
- Reintam Blaser A, Regli A, De Keulenaer B, Kimball EJ, Starkopf L, Davis WA, et al. Incidence, risk factors, and outcomes of intra-abdominal hypertension in critically ill patients—a prospective multicenter study (IROI Study) Crit Care Med. 2019;47:535–542. doi: 10.1097/CCM.0000000000003623. - DOI - PMC - PubMed
-
- Malbrain MLNG, Chiumello D, Cesana BM, Reintam Blaser A, Starkopf J, Sugrue M, et al. A systematic review and individual patient data meta-analysis on intra-abdominal hypertension in critically ill patients: the wake-up project. World initiative on Abdominal Hypertension Epidemiology, a Unifying Project (WAKE-Up!) Minerva Anestesiol. 2014;80:293–306. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
