Safety and Efficacy of Semorinemab in Individuals With Prodromal to Mild Alzheimer Disease: A Randomized Clinical Trial
- PMID: 35696185
- PMCID: PMC9194753
- DOI: 10.1001/jamaneurol.2022.1375
Safety and Efficacy of Semorinemab in Individuals With Prodromal to Mild Alzheimer Disease: A Randomized Clinical Trial
Abstract
Importance: Neurofibrillary tangles composed of aggregated tau protein are one of the neuropathological hallmarks of Alzheimer disease (AD) and correlate with clinical disease severity. Monoclonal antibodies targeting tau may have the potential to ameliorate AD progression by slowing or stopping the spread and/or accumulation of pathological tau.
Objective: To evaluate the safety and efficacy of the monoclonal anti-tau antibody semorinemab in prodromal to mild AD.
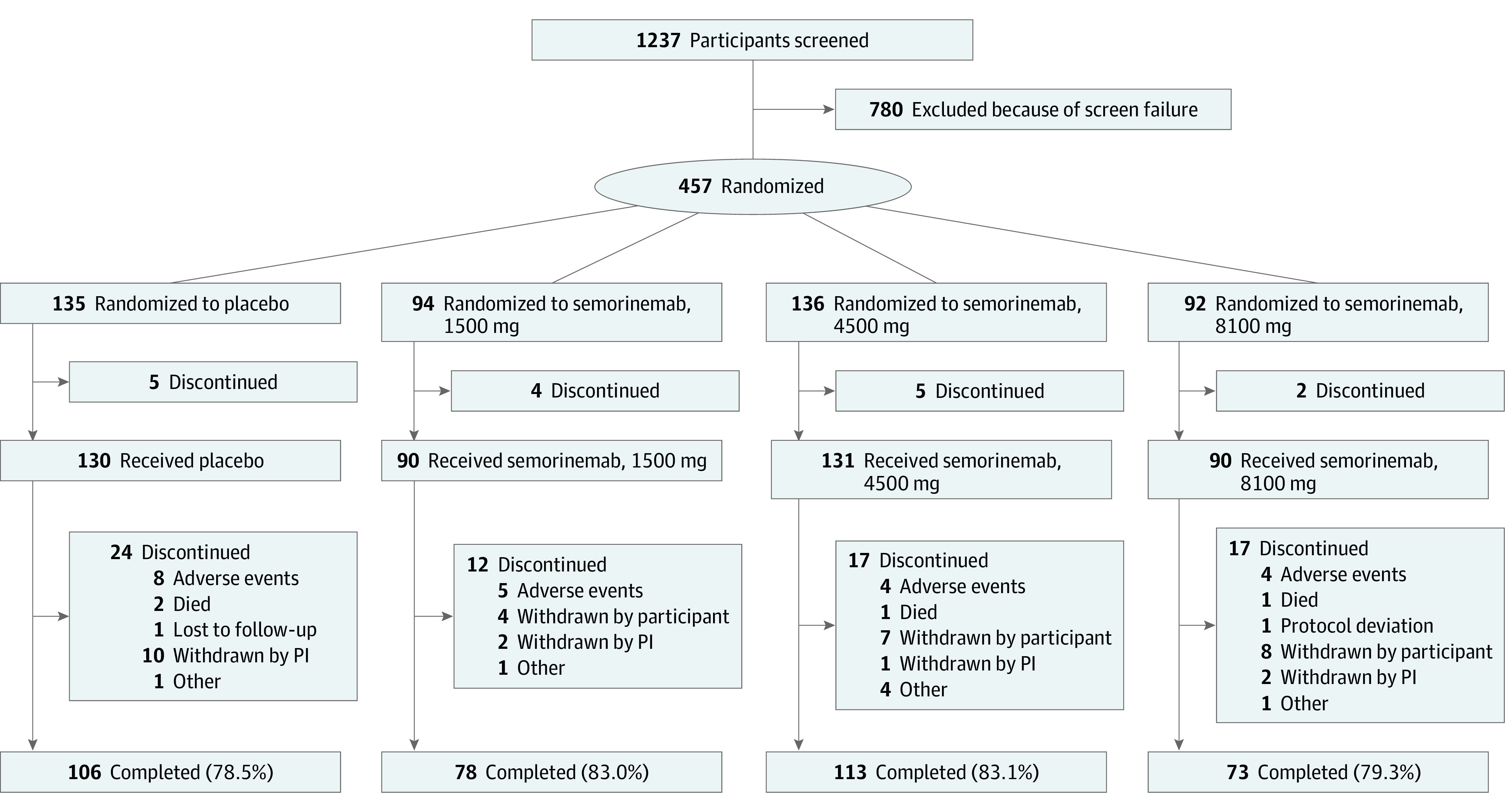
Design, setting, and participants: This phase 2 randomized, double-blind, placebo-controlled, parallel-group clinical trial was conducted between October 18, 2017, and July 16, 2020, at 97 sites in North America, Europe, and Australia. Individuals aged 50 to 80 years (inclusive) with prodromal to mild AD, Mini-Mental State Examination scores between 20 and 30 (inclusive), and confirmed β-amyloid pathology (by positron emission tomography or cerebrospinal fluid) were included.
Interventions: During the 73-week blinded study period, participants received intravenous infusions of placebo or semorinemab (1500 mg, 4500 mg, or 8100 mg) every 2 weeks for the first 3 infusions and every 4 weeks thereafter.
Main outcomes and measures: The primary outcomes were change from baseline on the Clinical Dementia Rating-Sum of Boxes score from baseline to week 73 and assessments of the safety and tolerability for semorinemab compared with placebo.
Results: In the modified intent-to-treat cohort (n = 422; mean [SD] age, 69.6 [7.0] years; 235 women [55.7%]), similar increases were seen on the Clinical Dementia Rating-Sum of Boxes score in the placebo (n = 126; Δ = 2.19 [95% CI, 1.74-2.63]) and semorinemab (1500 mg: n = 86; Δ = 2.36 [95% CI, 1.83-2.89]; 4500 mg: n = 126; Δ = 2.36 [95% CI, 1.92-2.79]; 8100 mg: n = 84; Δ = 2.41 [95% CI, 1.88-2.94]) arms. In the safety-evaluable cohort (n = 441), similar proportions of participants experienced adverse events in the placebo (130 [93.1%]) and semorinemab (1500 mg: 89 [88.8%]; 4500 mg: 132 [94.7%]; 8100 mg: 90 [92.2%]) arms.
Conclusions and relevance: In participants with prodromal to mild AD in this randomized clinical trial, semorinemab did not slow clinical AD progression compared with placebo throughout the 73-week study period but did demonstrate an acceptable and well-tolerated safety profile. Additional studies of anti-tau antibodies may be needed to determine the clinical utility of this therapeutic approach.
Trial registration: ClinicalTrials.gov Identifier: NCT03289143.
Conflict of interest statement
Figures