

TDP-43 Pathology Exacerbates Cognitive Decline in Primary Age-Related Tauopathy
- PMID: 35696592
- PMCID: PMC9391297
- DOI: 10.1002/ana.26438
TDP-43 Pathology Exacerbates Cognitive Decline in Primary Age-Related Tauopathy
Abstract
Objective: Primary age-related tauopathy (PART) refers to tau neurofibrillary tangles restricted largely to the medial temporal lobe in the absence of significant beta-amyloid plaques. PART has been associated with cognitive impairment, but contributions from concomitant limbic age-related TDP-43 encephalopathy neuropathologic change (LATE-NC) are underappreciated.
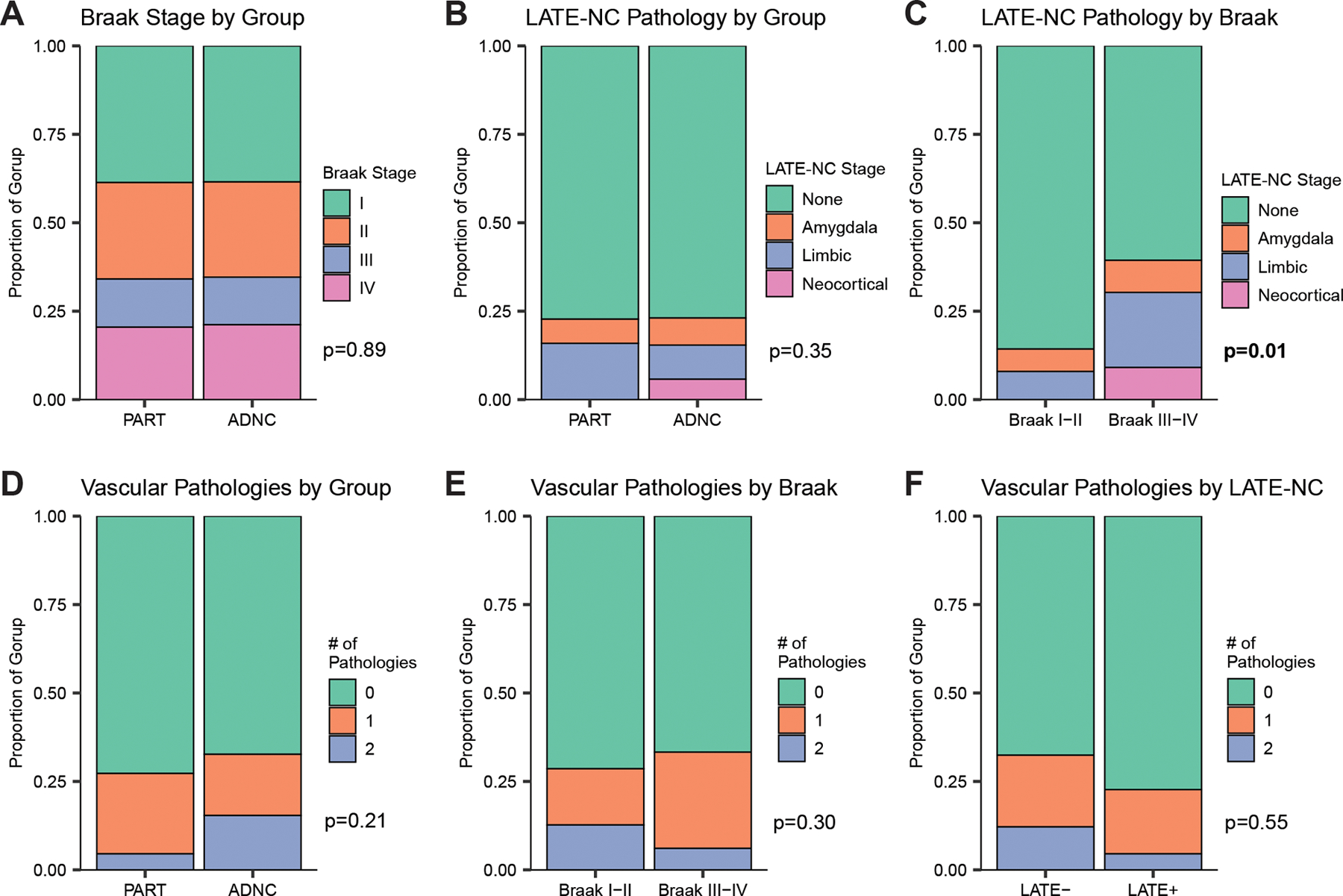
Methods: We compare prevalence of LATE-NC and vascular copathologies in age- and Braak-matched patients with PART (n = 45, Braak stage I-IV, Thal phase 0-2) or early stage Alzheimer disease neuropathologic change (ADNC; n = 51, Braak I-IV, Thal 3-5), and examine their influence on clinical and cognitive decline.
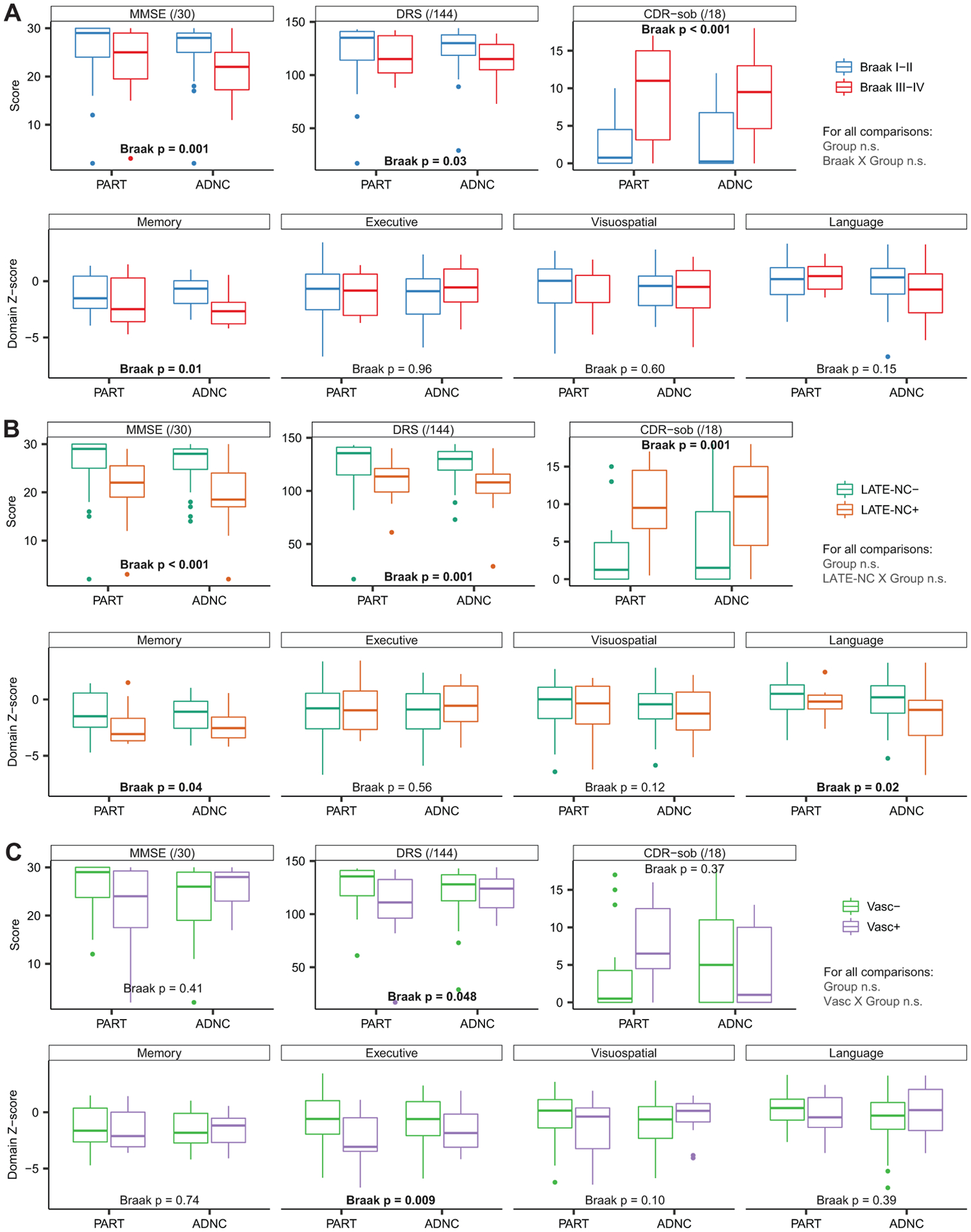
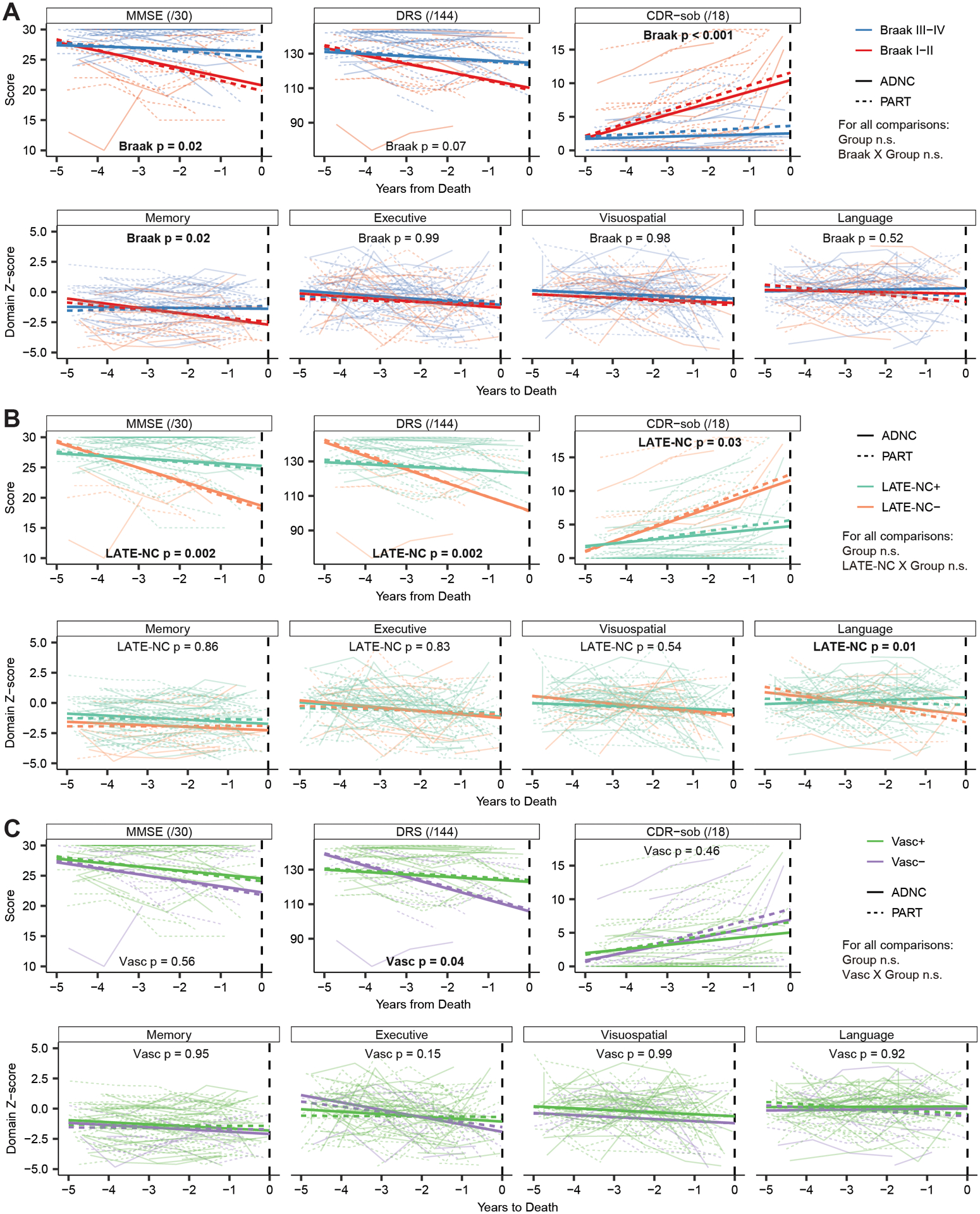
Results: Concomitant LATE-NC and vascular pathology were equally common, and cognition was equally impaired, in PART (Mini-Mental State Examination [MMSE] = 24.8 ± 6.9) and ADNC (MMSE = 24.2 ± 6.0). Patients with LATE-NC were more impaired than those without LATE-NC on the MMSE (by 5.8 points, 95% confidence interval [CI] = 3.0-8.6), Mattis Dementia Rating Scale (DRS; 17.5 points, 95% CI = 7.1-27.9), Clinical Dementia Rating, sum of boxes scale (CDR-sob; 5.2 points, 95% CI = 2.1-8.2), memory composite (0.8 standard deviations [SD], 95% CI = 0.1-1.6), and language composite (1.1 SD, 95% CI = 0.2-2.0), and more likely to receive a dementia diagnosis (odds ratio = 4.8, 95% CI = 1.5-18.0). Those with vascular pathology performed worse than those without on the DRS (by 10.2 points, 95% CI = 0.1-20.3) and executive composite (1.3 SD, 95% CI = 0.3-2.3). Cognition declined similarly in PART and ADNC over the 5 years preceding death; however, LATE-NC was associated with more rapid decline on the MMSE (β = 1.9, 95% CI = 0.9-3.0), DRS (β = 7.8, 95% CI = 3.4-12.7), CDR-sob (β = 1.9, 95% CI = 0.4-3.7), language composite (β = 0.5 SD, 95% CI = 0.1-0.8), and vascular pathology with more rapid decline on the DRS (β = 5.2, 95% CI = 0.6-10.2).
Interpretation: LATE-NC, and to a lesser extent vascular copathology, exacerbate cognitive impairment and decline in PART and early stage ADNC. ANN NEUROL 2022;92:425-438.
© 2022 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest:
All authors have nothing to report.
Figures

References
-
- Nelson PT, Abner EL, Schmitt FA, et al. Brains with medial temporal lobe neurofibrillary tangles but no neuritic amyloid plaques are a diagnostic dilemma but may have pathogenetic aspects distinct from Alzheimer disease. Journal of neuropathology and experimental neurology 2009;68(7):774–84. - PMC - PubMed
-
- Ikeda K, Akiyama H, Arai T, et al. Clinical Aspects of ‘Senile Dementia of the Tangle Type’ – A Subset of Dementia in the Senium Separable from Late-Onset Alzheimer’s Disease. Dement Geriatr Cogn 1999;10(1):6–11. - PubMed
-
- Itoh Y, Yamada M, Yoshida R, et al. Dementia Characterized by Abundant Neurofibrillary Tangles and Scarce Senile Plaques: A Quantitative Pathological Study. Eur Neurol 1996;36(2):94–97. - PubMed
-
- Bancher C, Jellinger KA. Neurofibrillary tangle predominant form of senile dementia of Alzheimer type: a rare subtype in very old subjects. Acta Neuropathol 1994;88(6):565–570. - PubMed
