

U.S. Trends in Registration for Medical Cannabis and Reasons for Use From 2016 to 2020 : An Observational Study
- PMID: 35696691
- PMCID: PMC10233658
- DOI: 10.7326/M22-0217
U.S. Trends in Registration for Medical Cannabis and Reasons for Use From 2016 to 2020 : An Observational Study
Abstract
Background: Cannabis policy liberalization has increased cannabis availability for medical or recreational purposes. Up-to-date trends in medical cannabis licensure can inform clinical policy and care.
Objective: To describe recent trends in medical cannabis licensure in the United States.
Design: Ecological study with repeated measures.
Setting: State registry data via state reports and data requests on medical cannabis licensure from 2016 to 2020.
Participants: Medical cannabis patients (persons with medical cannabis licenses) in the United States.
Measurements: Total patient volume, patients per 10 000 of total population, and patient-reported qualifying conditions (that is, symptoms or conditions qualifying patients for licensure)-including whether these symptoms align with current therapeutic evidence of cannabis-cannabinoid efficacy.
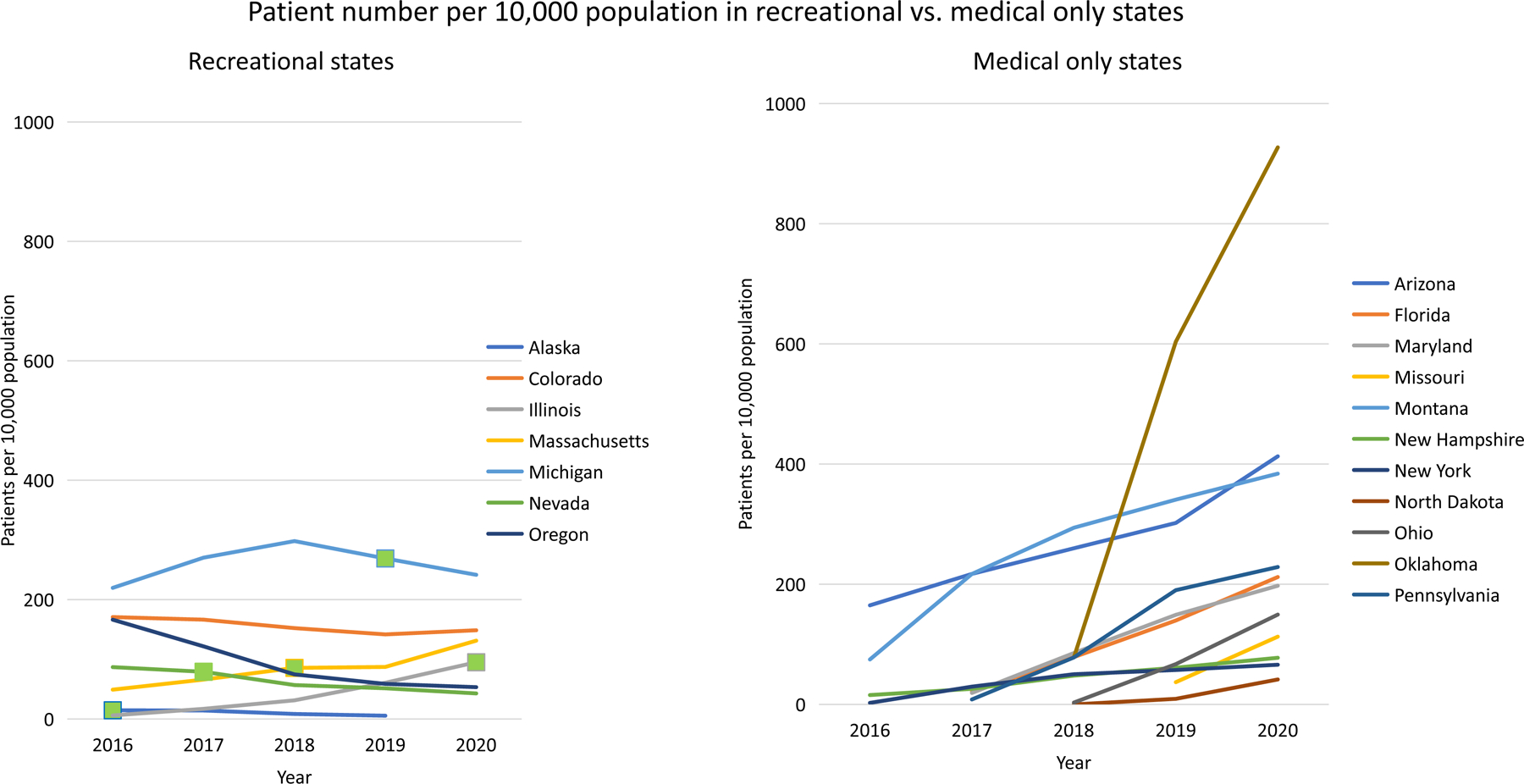
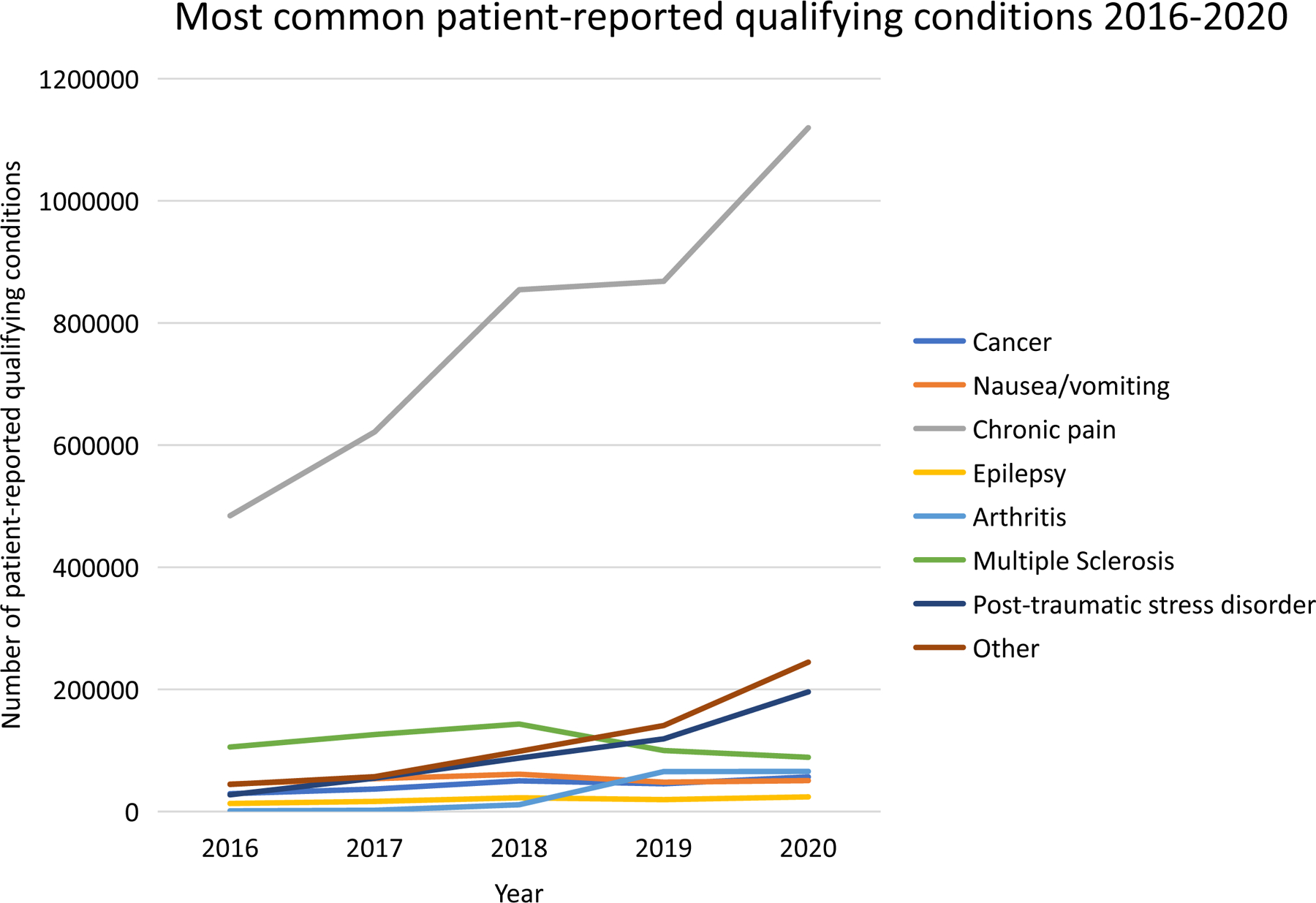
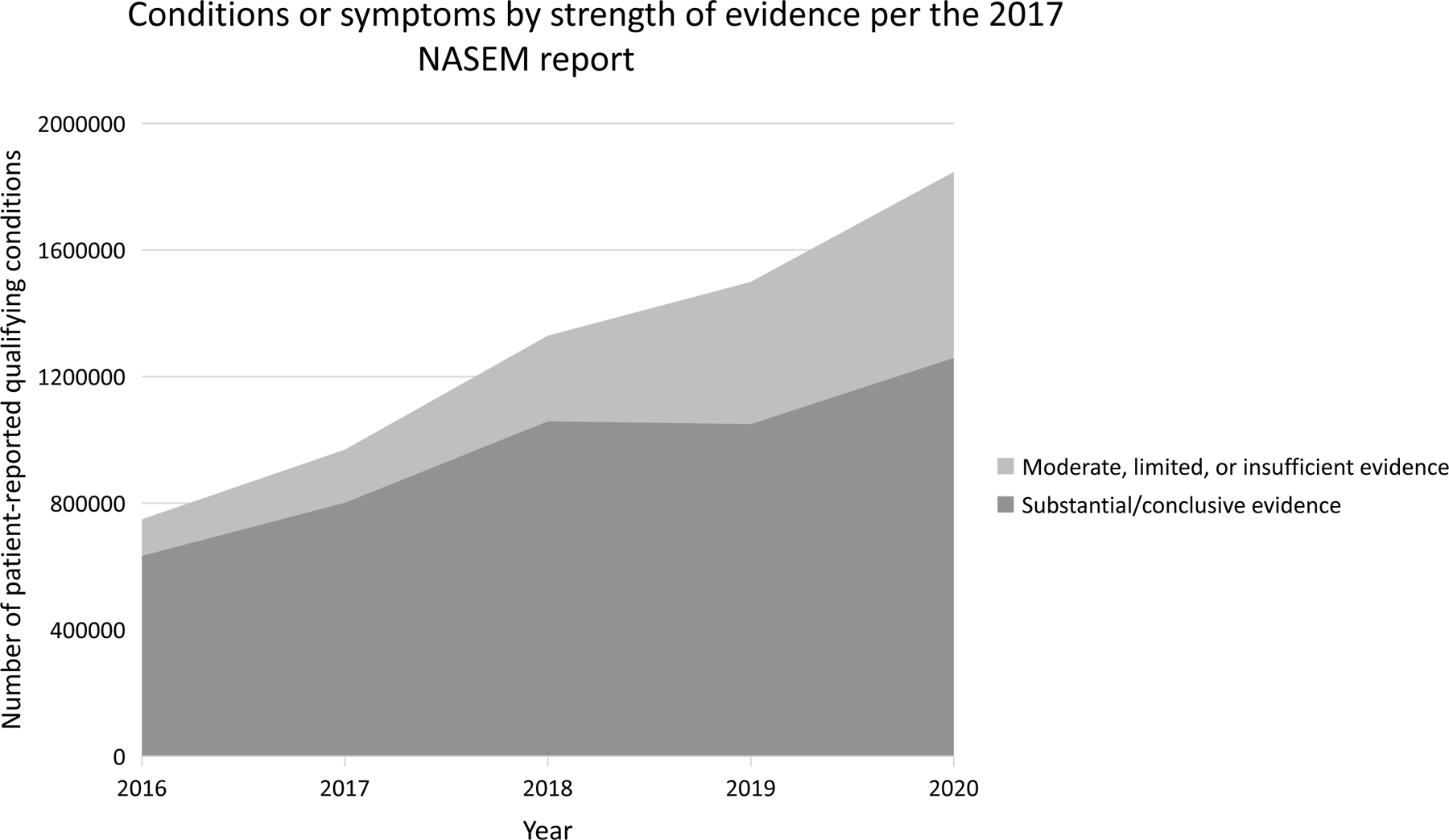
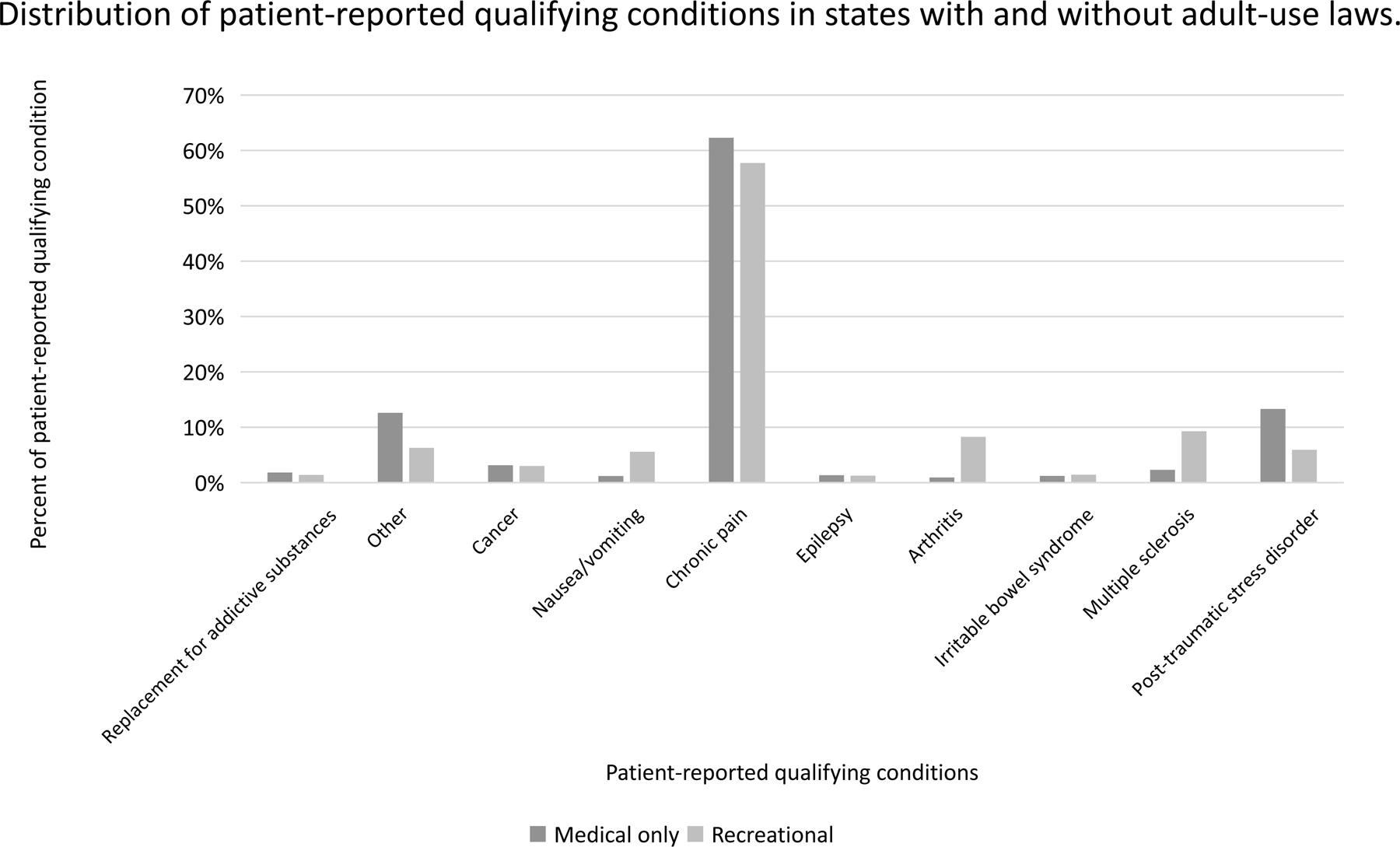
Results: In 2020, 26 states and Washington, DC reported patient numbers, and 19 states reported patient-reported qualifying conditions. Total enrolled patients increased approximately 4.5-fold from 678 408 in 2016 to 2 974 433 in 2020. Patients per 10 000 total population generally increased from 2016 to 2020, most dramatically in Oklahoma (927.1 patients per 10 000 population). However, enrollment increased in states without recreational legalization (that is, medical-only states), whereas enrollment decreased in 5 of 7 with recreational legalization (that is, recreational states). In 2020, 68.2% of patient-reported qualifying conditions had substantial or conclusive evidence of therapeutic value versus 84.6% in 2016. Chronic pain was the most common patient-reported qualifying condition in 2020 (60.6%), followed by posttraumatic stress disorder (10.6%).
Limitation: Missing state data; lack of rationale for discontinuing medical cannabis licensure.
Conclusion: Enrollment in medical cannabis programs approximately increased 4.5-fold from 2016 to 2020, although enrollment decreased in recreational states. Use for conditions or symptoms without a strong evidence basis increased from 15.4% (2016) to 31.8% (2020). Thoughtful regulatory and clinical strategies are needed to effectively manage this rapidly changing landscape.
Primary funding source: National Institute on Drug Abuse of the National Institutes of Health.
Figures
References
-
- National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington (DC); 2017. - PubMed
-
- Haffajee RL, MacCoun RJ, Mello MM. Behind Schedule - Reconciling Federal and State Marijuana Policy. N Engl J Med 2018;379(6):501–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical