

Chronic lung lesions in COVID-19 survivors: predictive clinical model
- PMID: 35697456
- PMCID: PMC9195157
- DOI: 10.1136/bmjopen-2021-059110
Chronic lung lesions in COVID-19 survivors: predictive clinical model
Abstract
Objective: This study aimed to propose a simple, accessible and low-cost predictive clinical model to detect lung lesions due to COVID-19 infection.
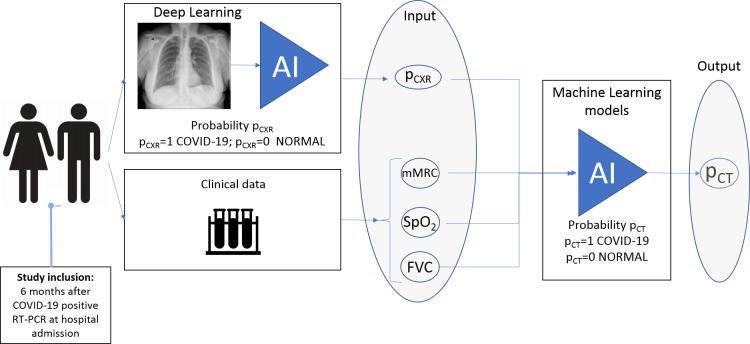
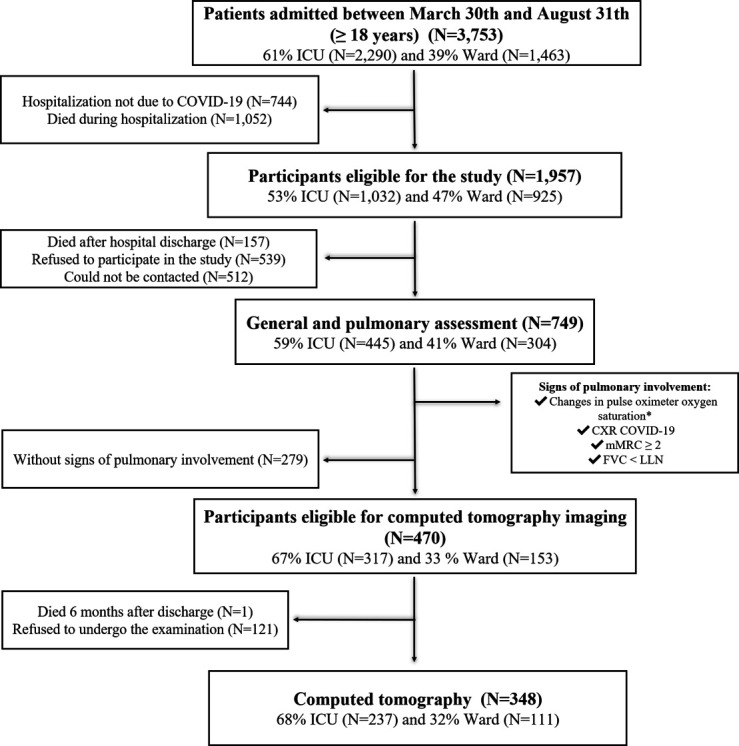
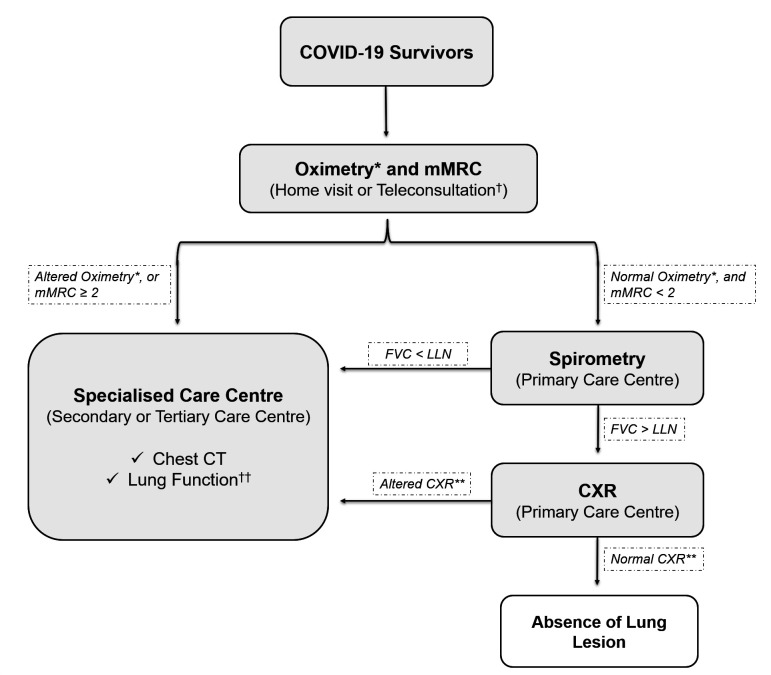
Design: This prospective cohort study included COVID-19 survivors hospitalised between 30 March 2020 and 31 August 2020 followed-up 6 months after hospital discharge. The pulmonary function was assessed using the modified Medical Research Council (mMRC) dyspnoea scale, oximetry (SpO2), spirometry (forced vital capacity (FVC)) and chest X-ray (CXR) during an in-person consultation. Patients with abnormalities in at least one of these parameters underwent chest CT. mMRC scale, SpO2, FVC and CXR findings were used to build a machine learning model for lung lesion detection on CT.
Setting: A tertiary hospital in Sao Paulo, Brazil.
Participants: 749 eligible RT-PCR-confirmed SARS-CoV-2-infected patients aged ≥18 years.
Primary outcome measure: A predictive clinical model for lung lesion detection on chest CT.
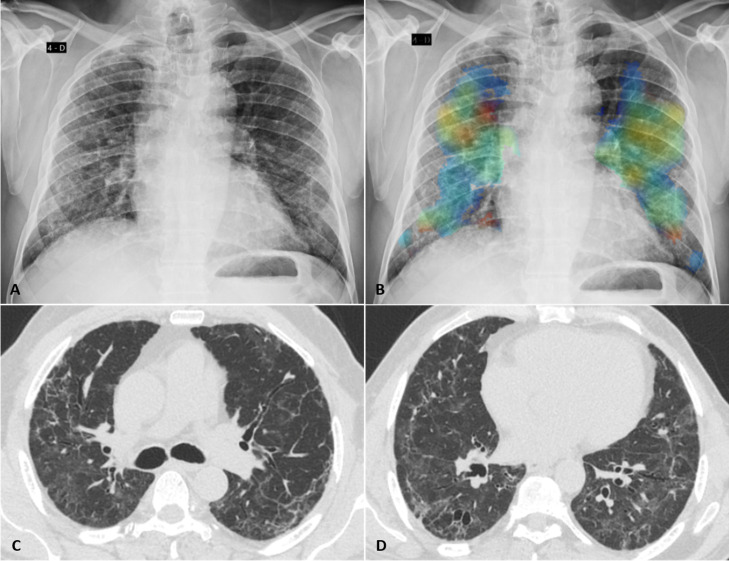
Results: There were 470 patients (63%) that had at least one sign of pulmonary involvement and were eligible for CT. Almost half of them (48%) had significant pulmonary abnormalities, including ground-glass opacities, parenchymal bands, reticulation, traction bronchiectasis and architectural distortion. The machine learning model, including the results of 257 patients with complete data on mMRC, SpO2, FVC, CXR and CT, accurately detected pulmonary lesions by the joint data of CXR, mMRC scale, SpO2 and FVC (sensitivity, 0.85±0.08; specificity, 0.70±0.06; F1-score, 0.79±0.06 and area under the curve, 0.80±0.07).
Conclusion: A predictive clinical model based on CXR, mMRC, oximetry and spirometry data can accurately screen patients with lung lesions after SARS-CoV-2 infection. Given that these examinations are highly accessible and low cost, this protocol can be automated and implemented in different countries for early detection of COVID-19 sequelae.
Keywords: COVID-19; chest imaging; respiratory medicine (see thoracic medicine).
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous