

Non-canonical WNT signalling in cardiovascular disease: mechanisms and therapeutic implications
- PMID: 35697779
- PMCID: PMC9191761
- DOI: 10.1038/s41569-022-00718-5
Non-canonical WNT signalling in cardiovascular disease: mechanisms and therapeutic implications
Abstract
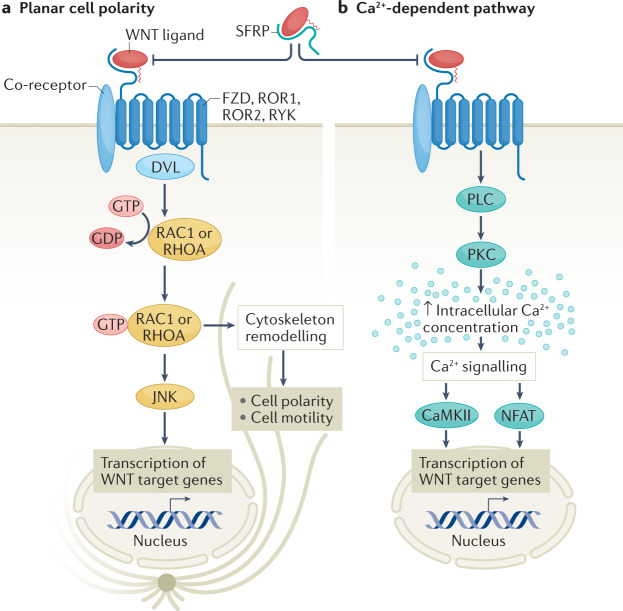
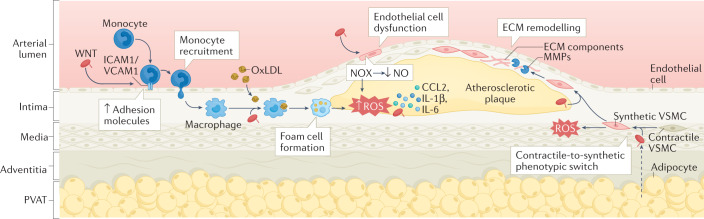
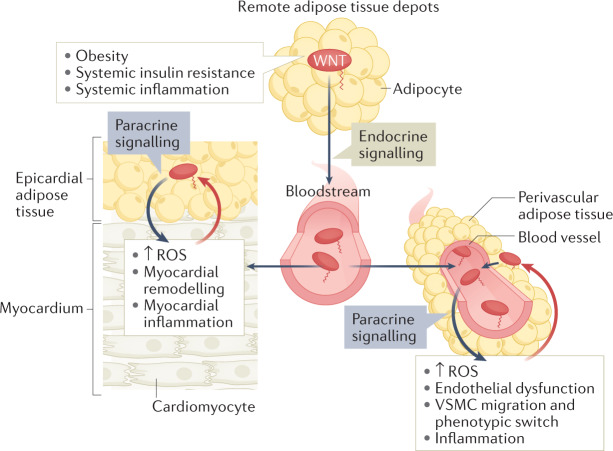
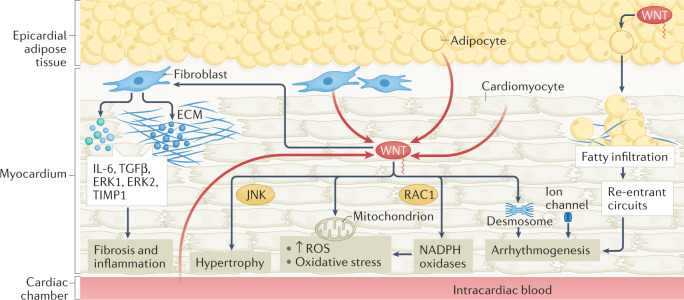
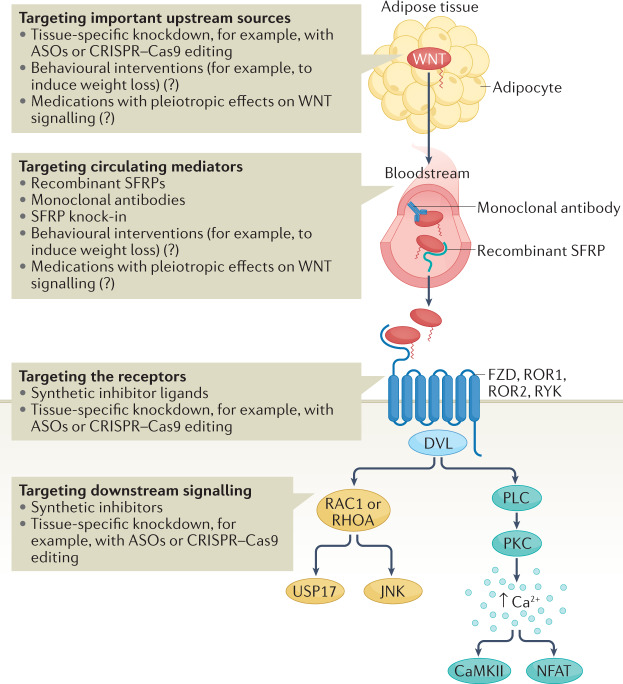
WNT signalling comprises a diverse spectrum of receptor-mediated pathways activated by a large family of WNT ligands and influencing fundamental biological processes. WNT signalling includes the β-catenin canonical pathway and the non-canonical pathways, namely the planar cell polarity and the calcium-dependent pathways. Advances over the past decade have linked non-canonical WNT signalling with key mechanisms of atherosclerosis, including oxidative stress, endothelial dysfunction, macrophage activation and vascular smooth muscle cell phenotype regulation. In addition, non-canonical WNT signalling is involved in crucial aspects of myocardial biology, from fibrosis to hypertrophy and oxidative stress. Importantly, non-canonical WNT signalling activation has complex effects in adipose tissue in the context of obesity, thereby potentially linking metabolic and vascular diseases. Tissue-specific targeting of non-canonical WNT signalling might be associated with substantial risks of off-target tumorigenesis, challenging its therapeutic potential. However, novel technologies, such as monoclonal antibodies, recombinant decoy receptors, tissue-specific gene silencing with small interfering RNAs and gene editing with CRISPR-Cas9, might enable more efficient therapeutic targeting of WNT signalling in the cardiovascular system. In this Review, we summarize the components of non-canonical WNT signalling, their links with the main mechanisms of atherosclerosis, heart failure and arrhythmias, and the rationale for targeting individual components of non-canonical WNT signalling for the treatment of cardiovascular disease.
© 2022. Springer Nature Limited.
Conflict of interest statement
C.A. is founder, shareholder and director of Caristo Diagnostics, a CT image analysis company. The other authors declare no competing interests.
Figures
References
-
- Hansson K. The heart of immunology: immune mechanisms in cardiovascular medicine. Cardiovasc. Res. 2021;117:e166–e168. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
