

Brain lesions disrupting addiction map to a common human brain circuit
- PMID: 35697842
- PMCID: PMC9205767
- DOI: 10.1038/s41591-022-01834-y
Brain lesions disrupting addiction map to a common human brain circuit
Abstract
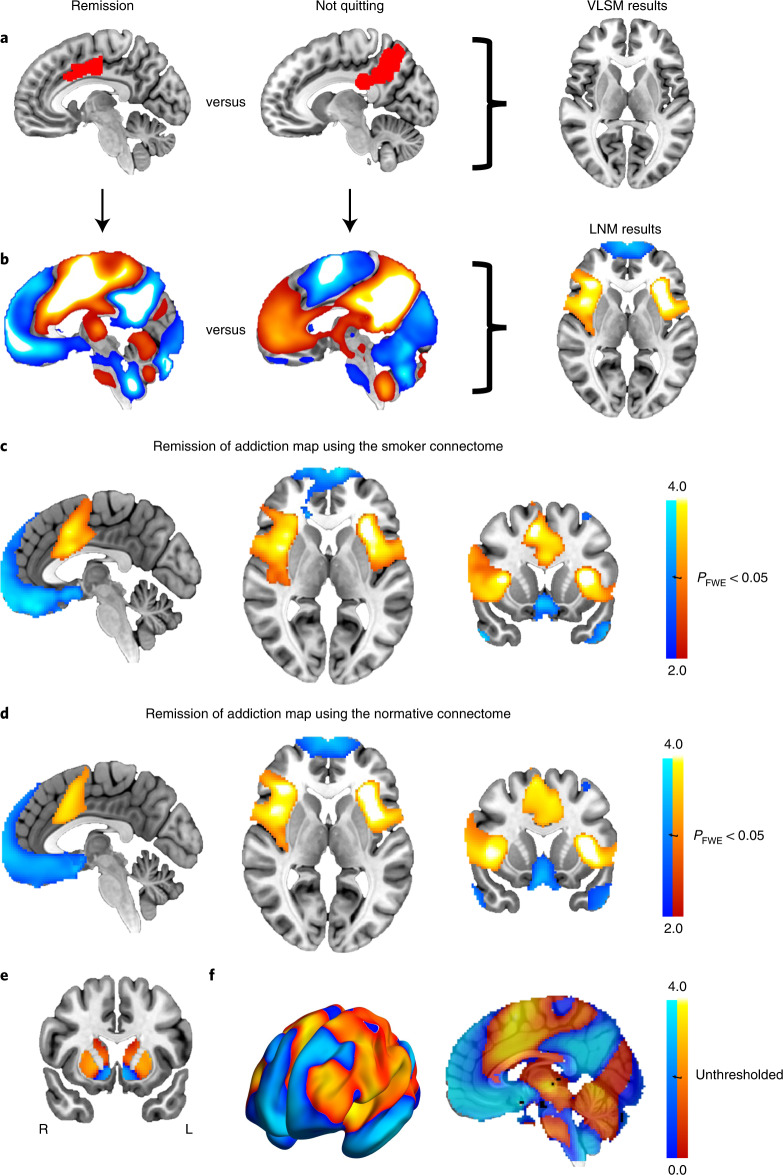
Drug addiction is a public health crisis for which new treatments are urgently needed. In rare cases, regional brain damage can lead to addiction remission. These cases may be used to identify therapeutic targets for neuromodulation. We analyzed two cohorts of patients addicted to smoking at the time of focal brain damage (cohort 1 n = 67; cohort 2 n = 62). Lesion locations were mapped to a brain atlas and the brain network functionally connected to each lesion location was computed using human connectome data (n = 1,000). Associations with addiction remission were identified. Generalizability was assessed using an independent cohort of patients with focal brain damage and alcohol addiction risk scores (n = 186). Specificity was assessed through comparison to 37 other neuropsychological variables. Lesions disrupting smoking addiction occurred in many different brain locations but were characterized by a specific pattern of brain connectivity. This pattern involved positive connectivity to the dorsal cingulate, lateral prefrontal cortex, and insula and negative connectivity to the medial prefrontal and temporal cortex. This circuit was reproducible across independent lesion cohorts, associated with reduced alcohol addiction risk, and specific to addiction metrics. Hubs that best matched the connectivity profile for addiction remission were the paracingulate gyrus, left frontal operculum, and medial fronto-polar cortex. We conclude that brain lesions disrupting addiction map to a specific human brain circuit and that hubs in this circuit provide testable targets for therapeutic neuromodulation.
© 2022. The Author(s).
Conflict of interest statement
M.D.F. and S.H.S. own patents on using brain connectivity to guide brain stimulation. M.D.F. and S.H.S. have received investigator-initiated research funding from Neuronetics, which is unrelated to the present work. The other authors declare no competing interests.
Figures



Similar articles
-
A Human Depression Circuit Derived From Focal Brain Lesions.Biol Psychiatry. 2019 Nov 15;86(10):749-758. doi: 10.1016/j.biopsych.2019.07.023. Epub 2019 Aug 2. Biol Psychiatry. 2019. PMID: 31561861 Free PMC article.
-
Mapping mania symptoms based on focal brain damage.J Clin Invest. 2020 Oct 1;130(10):5209-5222. doi: 10.1172/JCI136096. J Clin Invest. 2020. PMID: 32831292 Free PMC article.
-
Finding the imposter: brain connectivity of lesions causing delusional misidentifications.Brain. 2017 Feb;140(2):497-507. doi: 10.1093/brain/aww288. Epub 2017 Jan 12. Brain. 2017. PMID: 28082298 Free PMC article.
-
Mapping holmes tremor circuit using the human brain connectome.Ann Neurol. 2019 Dec;86(6):812-820. doi: 10.1002/ana.25618. Epub 2019 Oct 30. Ann Neurol. 2019. PMID: 31614012 Free PMC article.
-
Lesion network mapping for symptom localization: recent developments and future directions.Curr Opin Neurol. 2022 Aug 1;35(4):453-459. doi: 10.1097/WCO.0000000000001085. Epub 2022 Jul 5. Curr Opin Neurol. 2022. PMID: 35788098 Free PMC article. Review.
Cited by
-
Forced Abstinence from Volitional Ethanol Intake Drives a Vulnerable Period of Hyperexcitability in BNST-Projecting Insular Cortex Neurons.J Neurosci. 2024 Jan 24;44(4):e1121232023. doi: 10.1523/JNEUROSCI.1121-23.2023. J Neurosci. 2024. PMID: 38050120 Free PMC article.
-
Multi-omics analysis reveals GABAergic dysfunction after traumatic brainstem injury in rats.Front Neurosci. 2022 Nov 23;16:1003300. doi: 10.3389/fnins.2022.1003300. eCollection 2022. Front Neurosci. 2022. PMID: 36507346 Free PMC article.
-
Remission of alcohol use disorder following traumatic brain injury with focal orbitofrontal cortex hemorrhage: case report and network mapping.Commun Med (Lond). 2025 Mar 12;5(1):69. doi: 10.1038/s43856-025-00760-7. Commun Med (Lond). 2025. PMID: 40075136 Free PMC article.
-
Theta Burst Stimulation in Patients With Methamphetamine Use Disorder: A Meta-Analysis and Systematic Review.medRxiv [Preprint]. 2025 Mar 24:2025.03.24.25324326. doi: 10.1101/2025.03.24.25324326. medRxiv. 2025. Update in: J Addict Dis. 2025 Aug 4:1-13. doi: 10.1080/10550887.2025.2541165. PMID: 40196239 Free PMC article. Updated. Preprint.
-
Association between vmPFC gray matter volume and smoking initiation in adolescents.Nat Commun. 2023 Aug 15;14(1):4684. doi: 10.1038/s41467-023-40079-2. Nat Commun. 2023. PMID: 37582920 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
- K23 MH120510/MH/NIMH NIH HHS/United States
- R01 AG054328/AG/NIA NIH HHS/United States
- P50 HD105351/HD/NICHD NIH HHS/United States
- K99 DA048085/DA/NIDA NIH HHS/United States
- R01 MH113929/MH/NIMH NIH HHS/United States
- R21 NS123813/NS/NINDS NIH HHS/United States
- L30 MH127717/MH/NIMH NIH HHS/United States
- R00 DA048085/DA/NIDA NIH HHS/United States
- R21 MH126271/MH/NIMH NIH HHS/United States
- K23 MH121657/MH/NIMH NIH HHS/United States
- R56 AG069086/AG/NIA NIH HHS/United States
- R01 NS114405/NS/NINDS NIH HHS/United States
- P50 HD103556/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
