

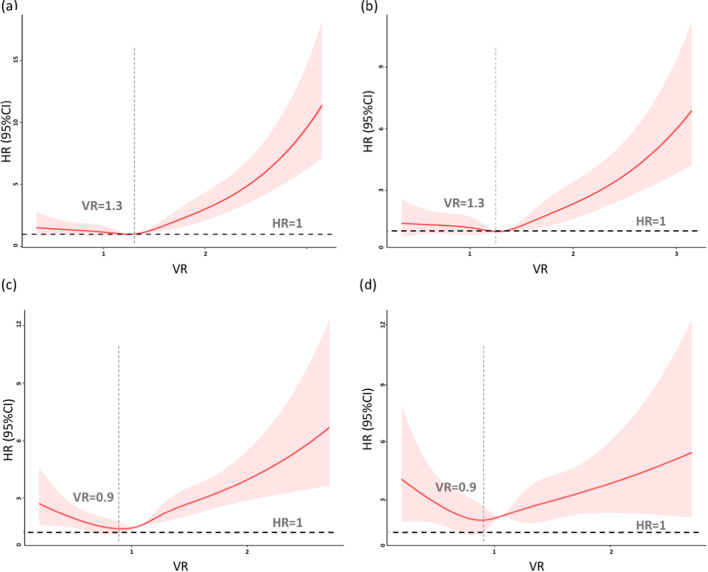
The relationship between ventilatory ratio (VR) and 28-day hospital mortality by restricted cubic splines (RCS) in 14,328 mechanically ventilated ICU patients
- PMID: 35698114
- PMCID: PMC9191763
- DOI: 10.1186/s12890-022-02019-6
The relationship between ventilatory ratio (VR) and 28-day hospital mortality by restricted cubic splines (RCS) in 14,328 mechanically ventilated ICU patients
Abstract
Background: Previous studies found that high levels of ventilatory ratio (VR) were associated with a poor prognosis due to worse ventilatory efficiency in acute respiratory distress syndrome patients. However, relatively few large studies have assessed the association between VR and intensive care unit (ICU) mortality in the general adult ventilated population.
Methods: The present study is a retrospective cohort study. Patients mechanically ventilated for more than 12 h were included. VR was calculated based on a previously reported formula. Restricted cubic spline models were used to fit the relationship between VR and mortality risks.
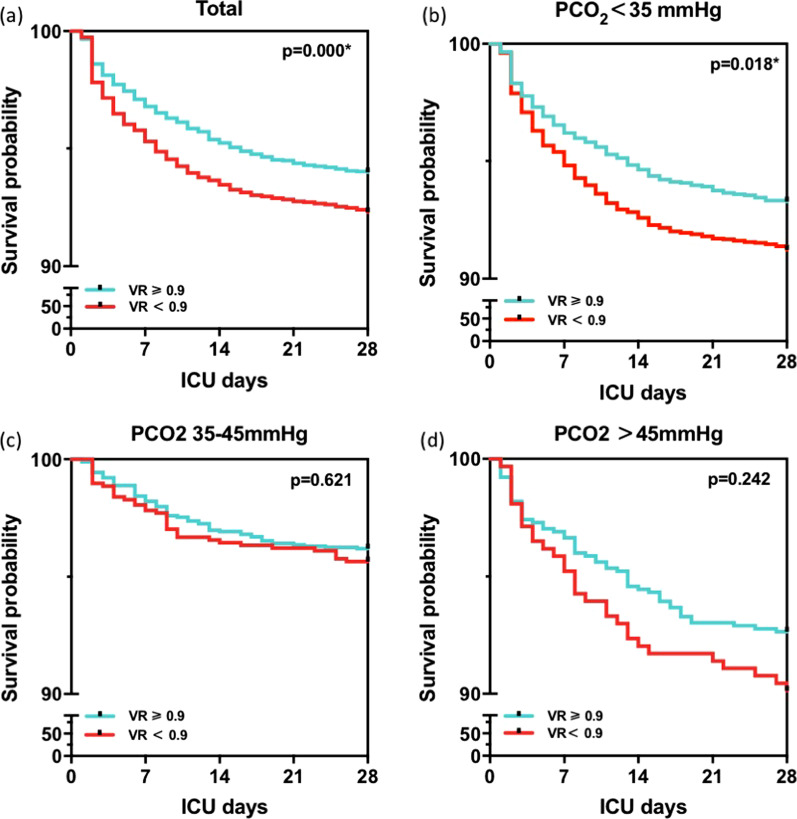
Results: A total of 14,328 mechanically ventilated ICU patients were included in the study, of which 1311 died within 28 days. The results of the study are as follows: (1) In the general adult ventilated population, VR was positively associated with 28-day mortality when VR ≥ 1.3 (increase of 0.1 per VR; HR 1.05, p < 0.001). The same tendency was also observed in the populations of severe hypoxemia with a PaO2/FiO2 (P/F) ratio < 200 mmHg. (2) However, in the population with a P/F ratio ≥ 200, a J-shaped dose-response association between VR and the risk of mortality was observed, with the risk of death positively associated with VR when VR ≥ 0.9 (10% increase in HR for every 0.1 increase in VR, p = 0.000) but negatively associated with VR when VR < 0.9 (10% decrease in HR for every 0.1 increase in VR, p = 0.034). In the population of P/F ratio ≥ 200 with VR less than 0.9, compared to the survival group, the nonsurvival group had a lower level PCO2 (33 mmHg [29.1, 37.9] vs. 34.4 mmHg [30.6, 38.5]), rather than a significant level of measured minute ventilation or P/F ratio.
Conclusions: VR was positively associated with the risk of death in the general ICU population; however, VR was inversely associated with 28-day mortality in the population with a P/F ratio ≥ 200 and low VR . Further research should investigate this relationship, and VR should be interpreted with caution in clinical practice.
Keywords: ICU mortality; Restricted cubic spline; Ventilatory ratio.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
