

Patterns of multidrug resistant organism acquisition in an adult specialist burns service: a retrospective review
- PMID: 35698209
- PMCID: PMC9195457
- DOI: 10.1186/s13756-022-01123-w
Patterns of multidrug resistant organism acquisition in an adult specialist burns service: a retrospective review
Abstract
Background: Multidrug resistant organisms (MDROs) occur more commonly in burns patients than in other hospital patients and are an increasingly frequent cause of burn-related mortality. We examined the incidence, trends and risk factors for MDRO acquisition in a specialist burns service housed in an open general surgical ward, and general intensive care unit.
Methods: We performed a retrospective study of adult patients admitted with an acute burn injury to our specialist statewide tertiary burns service between July 2014 and October 2020. We linked patient demographics, injury, treatment, and outcome details from our prospective burns service registry to microbiology and antimicrobial prescribing data. The outcome of interest was first MDRO detection, stratified into the following groups of interest: methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), two groups of Pseudomonas (carbapenem resistant, and piperacillin-tazobactam or cefepime resistant), carbapenem-resistant Acinetobacter species, Stenotrophomonas maltophilia, carbapenem-resistant Enterobacteriaceae (CRE), and extended-spectrum beta-lactamase producing Enterobacteriaceae (ESBL-PE). We used a Cox proportional hazards model to evaluate the association between antibiotic exposure and MDRO acquisition.
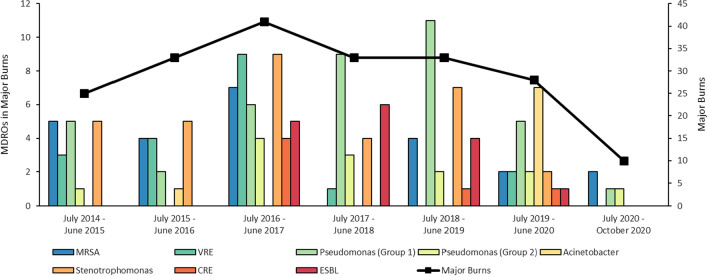
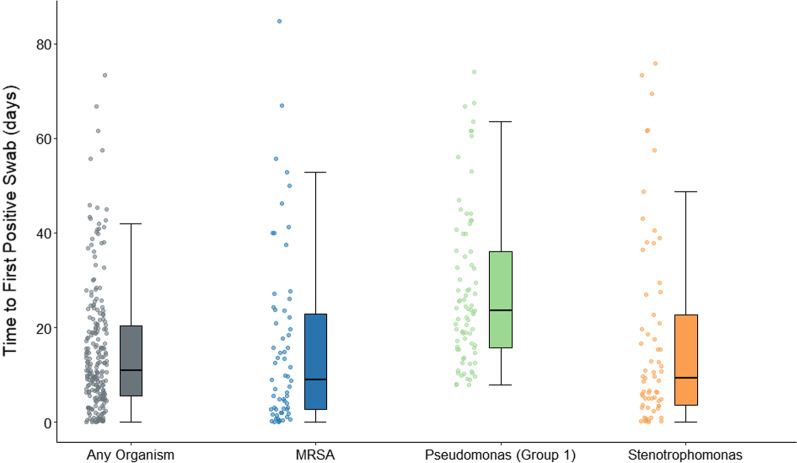
Results: There were 2,036 acute admissions, of which 230 (11.3%) had at least one MDRO isolated from clinical specimens, most frequently wound swabs. While acquisition rates of individual MDRO groups varied over the study period, acquisition rate of any MDRO was reasonably stable over time. Carbapenem-resistant Pseudomonas was acquired at the highest rate over the study period (3.5/1000 patient days). The 12.8% (29/226) of MDROs isolated within 48 h were predominantly MRSA and Stenotrophomonas. Median (IQR) time from admission to MDRO detection was 10.9 (5.6-20.5) days, ranging from 9.8 (2.7-24.2) for MRSA to 23.6 (15.7-36.0) for carbapenem-resistant P. aeruginosa. Patients with MDROs were older, had more extensive burns, longer length of stay, and were more likely to have operative burn management. We were unable to detect a relationship between antibiotic exposure and emergence of MDROs.
Conclusions: MDROs are a common and consistent presence in our burns unit. The pattern of acquisition suggests various causes, including introduction from the community and nosocomial spread. More regular surveillance of incidence and targeted interventions may decrease their prevalence, and limit the development of invasive infection.
Keywords: Burn injury; Multi-drug resistant bacteria.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Van Langeveld I, Gagnon RC, Conrad PF, Gamelli RL, Martin B, Choudhry MA, et al. Multiple-drug resistance in burn patients: a retrospective study on the impact of antibiotic resistance on survival and length of stay. J Burn Care Res. 2017;38:99–105. doi: 10.1097/BCR.0000000000000479. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
